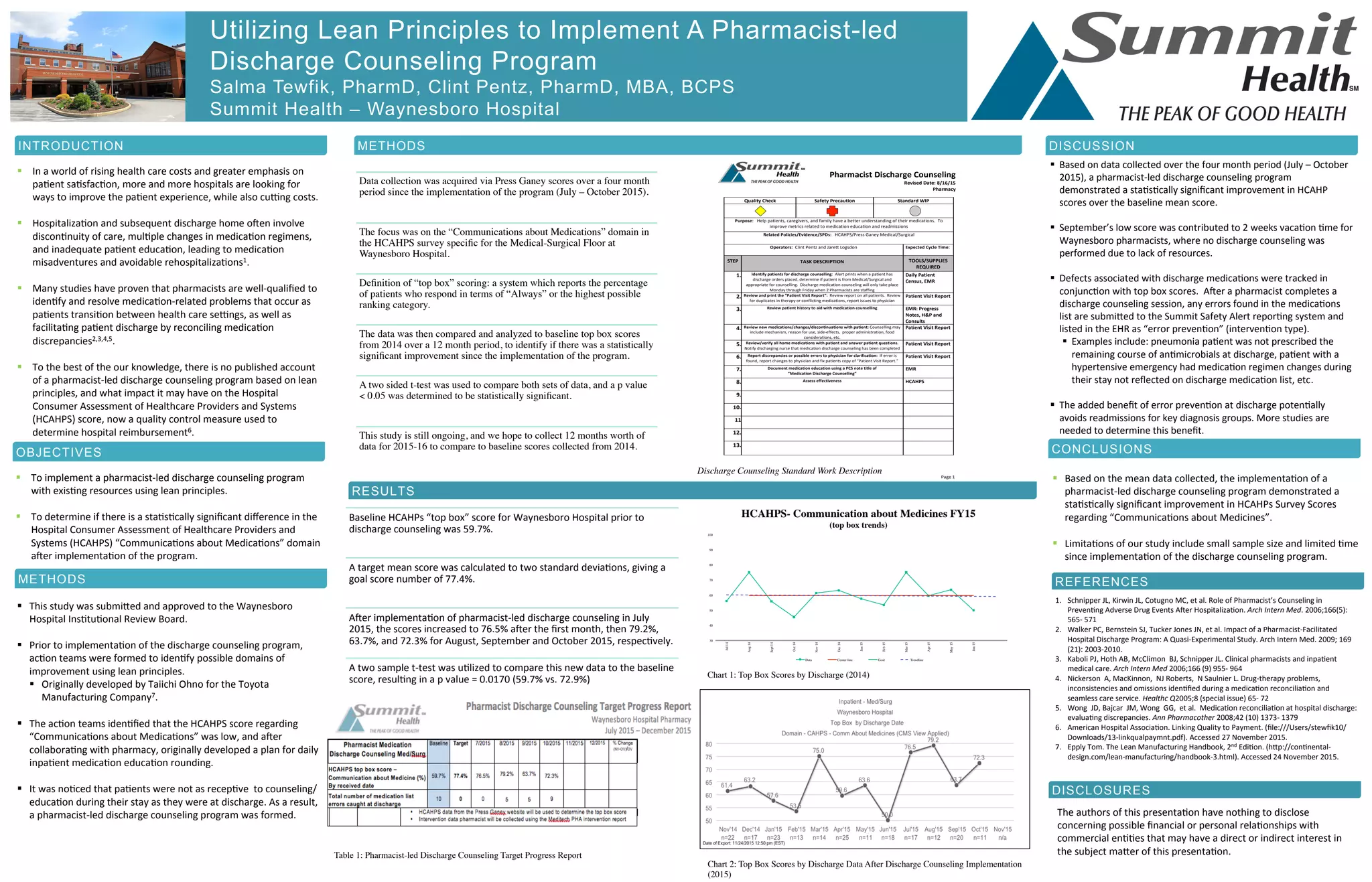
The document describes a study conducted at Waynesboro Hospital to implement a pharmacist-led discharge counseling program using lean principles. The objectives were to utilize existing resources to conduct discharge counseling and determine if it improved HCAHPS scores regarding "Communications about Medications". After implementing the program, the HCAHPS scores for that domain increased significantly from a baseline of 59.7% to a mean of 72.9% over four months, representing a statistically significant improvement with a p-value of 0.0170. The results indicate pharmacist-led discharge counseling can successfully enhance patient education and experience regarding medications.













































![Chapter 1[1]](https://cdn.slidesharecdn.com/ss_thumbnails/chapter11-150306090427-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)















