Downloaded 11 times





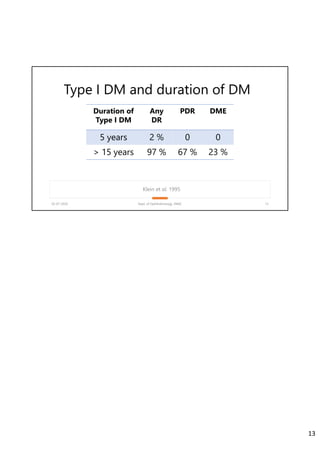
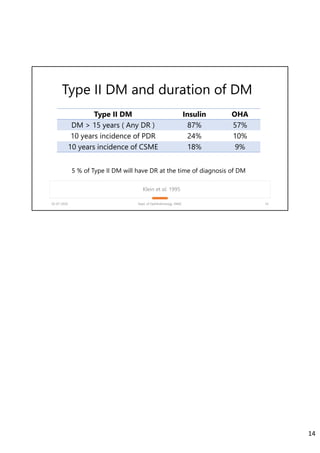








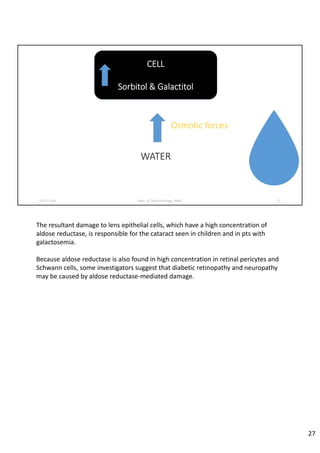









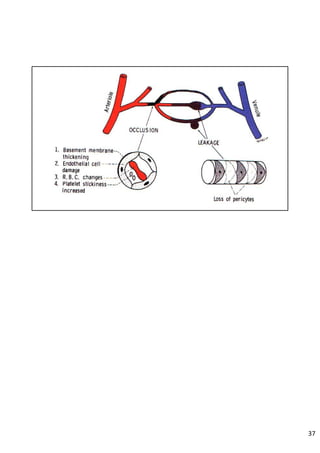

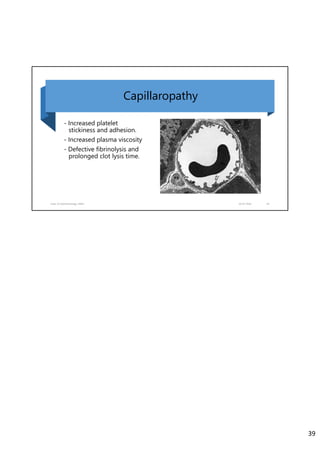



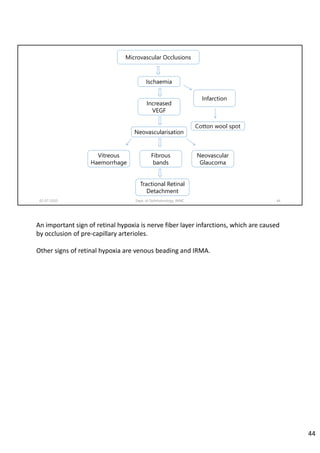
















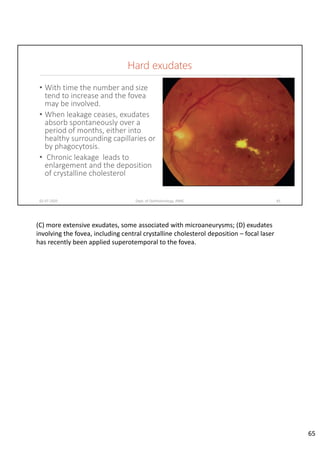





































































Diabetic retinopathy is caused by damage to the blood vessels in the retina from chronic hyperglycemia. It is the most common retinal vascular disease and a leading cause of vision loss. The risk and severity of diabetic retinopathy increases with longer duration of diabetes, poorer blood glucose control, and presence of other complications like hypertension. The pathogenesis involves microvascular changes like capillary non-perfusion and death of pericytes, as well as increased vascular permeability and neo-vascularization due to elevated levels of vasoactive growth factors. Strict control of blood glucose and other cardiovascular risk factors can help prevent and slow the progression of this vision-threatening condition.