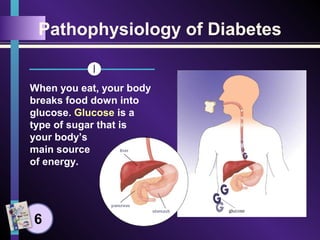
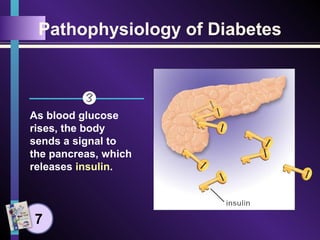
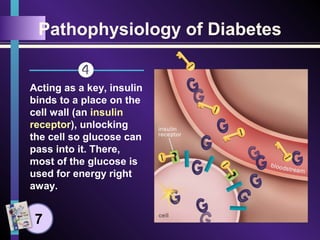
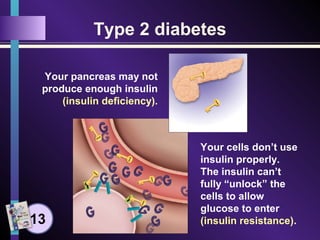
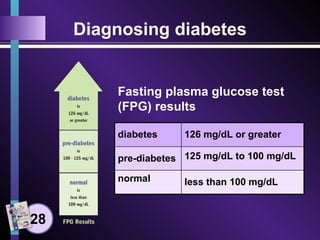
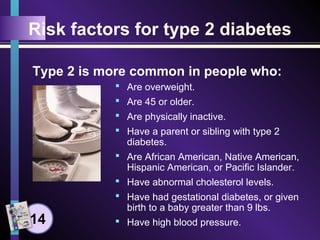
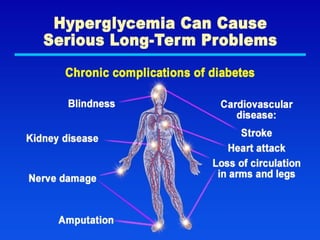
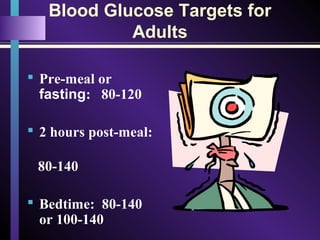
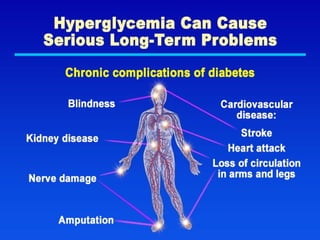
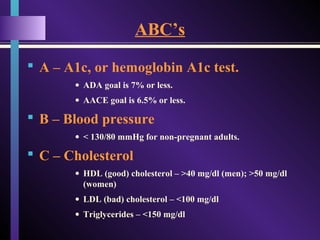
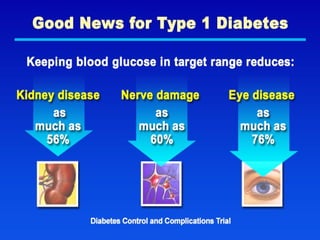
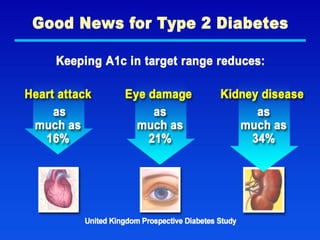
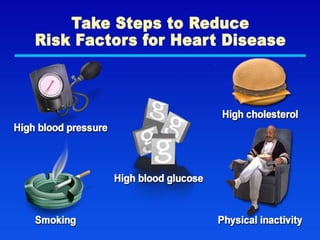
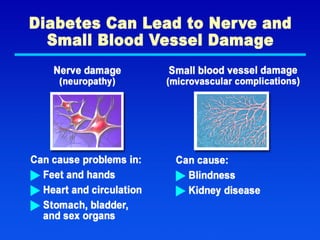
Diabetes affects 25.8 million adults in the U.S., with multiple types, including Type I, Type II, and gestational diabetes, characterized by issues with insulin production and utilization. Key management strategies involve monitoring blood glucose, taking medications, following meal plans, and maintaining physical activity to avoid long-term complications like cardiovascular disease. Diagnosis depends on blood glucose levels, with risk factors including obesity, age, and family history.







































![latest in diabetes ppt 8.12.21 [Autosaved].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/diabetesppt8-250113164357-608e4fb0-thumbnail.jpg?width=640&height=640&fit=bounds)



















![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





