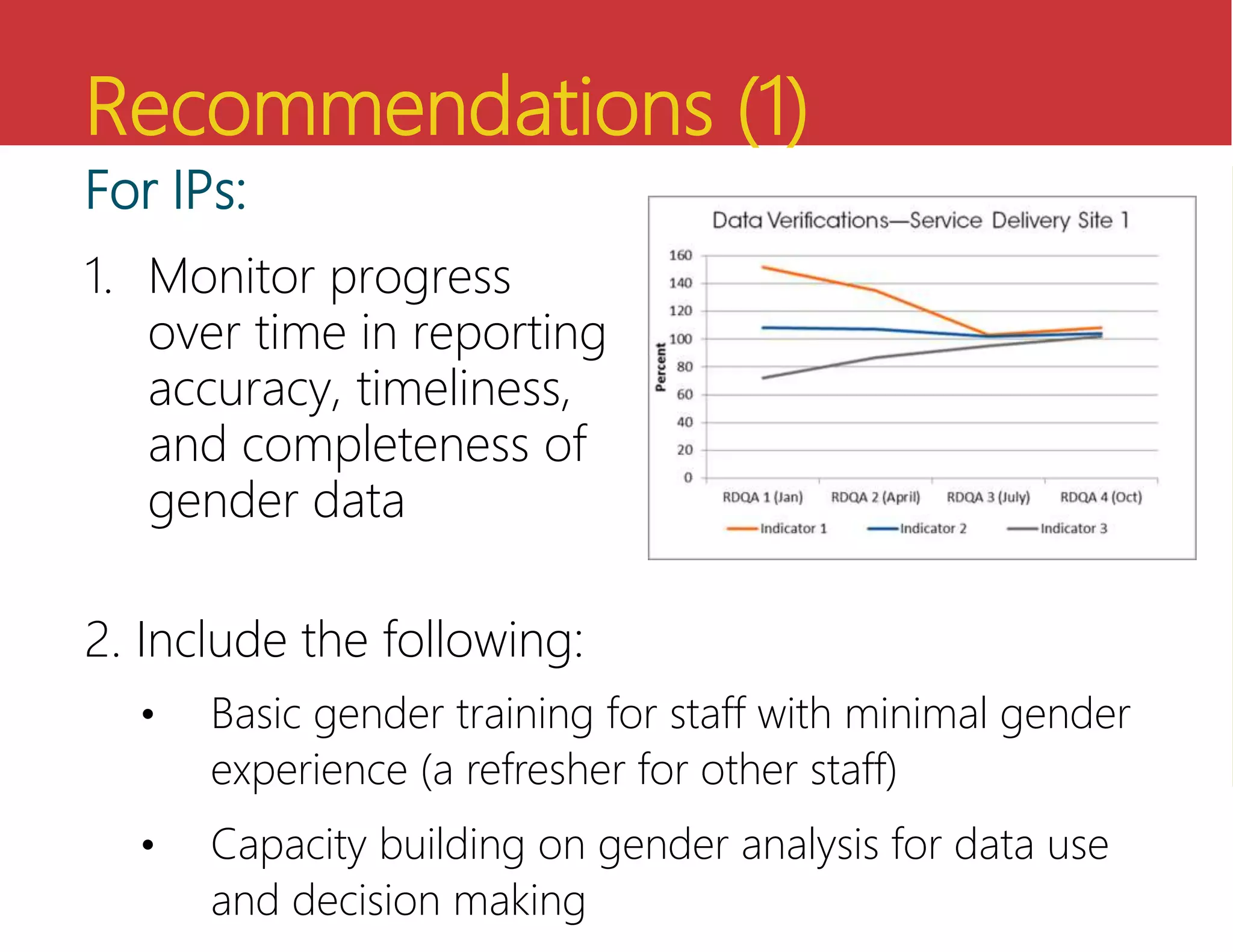
The document discusses the importance and challenges of collecting and using sex- and age-disaggregated data in health systems, highlighting the significant impact of gender inequality on health outcomes. It identifies barriers and facilitators to the availability and effective use of such data, emphasizing the need for improved training, advocacy, and systems to enhance gender integration in health information. Recommendations for enhancing data disaggregation and the use of gender-sensitive indicators are also provided.