DELAYED RELEASE DRUGDELIVERY SYSTEMS
The oral administration of drugs represents the most common way of drug
application due to its high patient acceptance. The major portion of the oral drug delivery
comprises of tablets, solid unit dosage forms, having higher patient acceptance. There is a
revolutionary improvement in the technology of both in conventional as well as
controlled drug delivery systems.
The immediate release drug delivery systems are particularly used to produce fast
therapeutic drug plasma levels. This results in reduction or loss in drug effectiveness or
also increased incidence of side effects. Modified release drug delivery systems include
the systems with pH dependent, extended, delayed or pulsed drug release. Sustained,
extended or prolonged release drug delivery devices, by contrast, are delayed release
dosage forms have to be distinguished from the ones mentioned as they exhibit a more or
less pronounced lag time before drug release.
A Delayed Release dosage form is designed to release the drug at a time other
than promptly after administration. Dosage forms can be designed to modify the
release of the drug over a given time or after the dosage form reaches the required
location.
Drug Delivery System:
Conventional drug delivery dosage forms include tablets, injectables, suspensions,
creams, ointments, liquids and aerosols are widely used now a day. The term drug
delivery can be defined as techniques that are used to get the therapeutic agents inside
the human body.
Conventional drug therapy requires periodic doses of therapeutic agents. These agents
are formulated to produce maximum stability, activity and bioavailability. For most
drugs, conventional methods of drug administration are effective, but some drugs are
unstable or toxic and have narrow therapeutic window. Conventional dosage forms are
associated with many side effects such as the initial dose may not be adequate enough to
reach the therapeutic range to elicit pharmacological response, some drugs possess
solubility problems. In such cases a method of continuous administration of therapeutic
2.
agent is desirableto maintain fixed plasma levels as shown in figure-1. Beside this the
repeated drug administration at the equal interval may result in severe side effect. These
problems of conventional dosage forms are overcome by controlled drug delivery
systems. Controlled drug delivery systems have a number of advantages over traditional
systems such as improved efficiency, reduced toxicity and improved patient convenience.
The main goal of controlled drug delivery systems is to improve the effectiveness of drug
therapies.
To overcome the disadvantages of conventional release dosage forms, the
formulations can be modified to provide either delayed release or extended release of
drugs. The USP and NF has defined a modified release dosage forms as one in which the
drug release characteristics of time course and/or location are chosen to accomplish
therapeutic or convenience objectives not offered by conventional dosage forms.
Modified-release products fall in two categories. One is extended-release dosage forms
which allow a reduction in dosing frequency or diminishes the fluctuation of drug levels
that observed on repeated administration of immediate-release dosage forms. Controlled
and sustained release products fall into this category. The second category is delayed-
release.
PDC-Time profile for CDDS
3.
Drug levels inthe blood with
a) Conventional drug delivery systems and
b) Controlled drug delivery systems
Controlled drug delivery is delivery of drug at a rate or at a location determined by
needs of body or disease state over a specified period of time.
The oral controlled release systems are classified as follows:
A) Continuous release systems
B) Delayed transit and continuous release systems
C) Delayed release systems
Delayed Release:
A Delayed Release dosage form is designed to release the drug at a time other than
promptly after administration. Dosage forms can be designed to modify the release of the
drug over a given time or after the dosage form reaches the required location.
Delayed Release oral dosage forms can control where the drug is released, e.g. when the
dosage form reaches the small intestine (enteric-coated dosage forms) or the colon
(colon-specific dosage forms). Delayed Release systems release a bolus of the drug after
a predetermined time in a predetermined location, i.e. they do not release the drug
immediately after ingestion, for example enteric-coated tablets, pulsatile-release capsules.
Delayed Release dosage forms are designed to provide spatial placement or
temporal targeted delivery of a drug to the distal human gut. Spatial placement relates to
targeting a drug to a specific organ or tissue, while temporal delivery refers to desired
rate of drug release to target tissue over a specified period of time. The primary aim of
using delayed release products is to protect the drug from gastric fluids, to reduce gastric
distress caused by drugs particularly irritating to the stomach or to facilitate
gastrointestinal transit for drugs that are better absorbed from intestine. Delayed Release
products are typically enteric-coated or targeted to the colon.
The oral route of drug delivery is typically considered the preferred and most
patient-convenience means of drug administration. The release of drug from an oral
dosage form may be intentionally delayed until it reaches the intestine.
4.
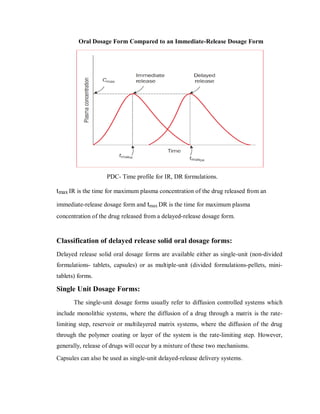
Oral Dosage FormCompared to an Immediate-Release Dosage Form
PDC- Time profile for IR, DR formulations.
tmax IR is the time for maximum plasma concentration of the drug released from an
immediate-release dosage form and tmax DR is the time for maximum plasma
concentration of the drug released from a delayed-release dosage form.
Classification of delayed release solid oral dosage forms:
Delayed release solid oral dosage forms are available either as single-unit (non-divided
formulations- tablets, capsules) or as multiple-unit (divided formulations-pellets, mini-
tablets) forms.
Single Unit Dosage Forms:
The single-unit dosage forms usually refer to diffusion controlled systems which
include monolithic systems, where the diffusion of a drug through a matrix is the rate-
limiting step, reservoir or multilayered matrix systems, where the diffusion of the drug
through the polymer coating or layer of the system is the rate-limiting step. However,
generally, release of drugs will occur by a mixture of these two mechanisms.
Capsules can also be used as single-unit delayed-release delivery systems.
5.
Multiple unit dosageforms :
Types of multiple unit dosage forms comprise
Pellets
Granules
Mini tablets and mini depots (dispersed and distributed throughout the gastrointestinal
tract when the capsule or tablet disintegrates)
Micro particles (Microspheres or Microcapsules) and Nano particles
Multiple unit tablets (divided at ingestion without loss of the depot effect, as the sub
unit act as self-contained depots).
Multi particulates are
filled into hard-shell gelatin capsules
compressed into tablets
suspended in liquids or
packed in sachets.
Significance of Delayed Release Systems:
The design of such system involves release of drugs only at a specific site in the
gastrointestinal tract. The drugs contained in such a system are those that are,
Destroyed in the stomach or by intestinal enzymes
Known to cause gastric distress
Absorbed from a specific intestinal site
Meant to exert local effect at a specific gastrointestinal site
In these cases drug release should be delayed until the dosage form has reached
the small intestine. Often polymers are used to achieve this aim. The dosage form (for
example, a tablet or the granules before tableting) can be coated with a suitable polymer.
The polymer dissolves as a function of pH, so when the dosage forms travel from the
low-pH environment of the stomach to the higher-pH environment of the small intestine,
the polymer coat dissolves and the drug can be released. Once this occurs, the release is
again immediate and the resulting plasma concentration versus time curve is similar to
the one for immediate release dosage forms.
6.
The two typesof delayed release systems are:
Intestinal Release System
Colonic Release System
Intestinal Release System:
A drug may be enteric coated for intestinal release for several known reasons such
as to prevent gastric irritation, prevent destabilization in gastric pH etc.
Colonic Release System:
Drugs are poorly absorbed through colon but may be delivered to such a site for
two reasons
Local action in the treatment of ulcerative colitis
Systemic absorption of protein and peptide drugs
The development of colon-specific drugs and dosage forms may be advantageous
for the treatment of local and systemic disease including colorectal cancer and Crohn’s
disease. Especially for peptide and protein drugs, this form of release may also be
advantageous for systemic administration given the more favourable pH conditions in the
colon compared to the stomach and the generally lower enzymatic activity compared to
the small intestine.
Advantage is taken of the fact that pH sensitive bioerodible polymers like poly
metha crylates release the medicament only at the alkaline pH of colon or use of
divinylbenzene cross-linked polymers that can be cleaved only by the azo reductase of
colonic bacteria to release free drug for local effect or systemic absorption.
General Considerations for Design of Formulations:
The proper selection of a formulation approach is dependent upon several important
factors, which are listed below.
Pathology and pattern of the disease, especially the affected parts of the lower GI
tract or physiology and physiological composition of the healthy colon if the formulation
is not intended for localized treatment.
Physicochemical and biopharmaceutical properties of the drug such as solubility,
stability and permeability at the intended site of delivery and the desired release profile of
the active ingredient.
7.
The mostcommon physiological factor considered in the design of delayed
release colonic formulations is pH gradient of the GI tract. In normal healthy subjects,
there is a progressive increase in luminal pH from the duodenum (pH = 6.6 + 0.5) to the
terminal ileum (pH = 7.5 + 0.4), a decrease in the cecum (pH = 6.4 + 0.4) and then a slow
rise from the right to the left colon with a final value of pH 7.0 + 0.7. Some reports
suggest that alterations in GI pH profiles may occur in patients with inflammatory bowel
disease, which should be considered in the development of delayed release formulations.
Approaches to Drug Delivery:
In recent years, a large number of solid formulations targeting the lower parts of the GI
tract, especially the colon, have been reported. These formulations may be broadly
divided into four types, which are
1. pH-dependent system designed to release a drug in response to change in pH,
2. Time controlled (or Time-dependent) system designed to release a drug after a
predetermined time,
3. Microbially-controlled system making use of the abundant entero bacteria in the
colon,
4. Enzyme-based systems – Prodrug, and
5. Pressure-dependent system making use of luminal pressure of the colon.
8.
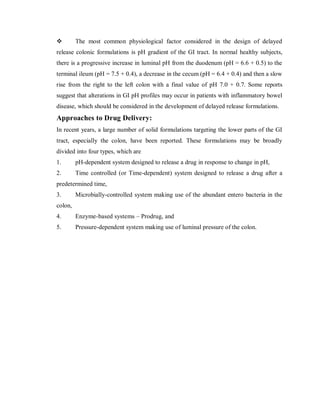
Threshold pH ofcommonly used polymers
Polymer Threshold pH
Eudragit®
L100
Eudragit®
S100
Eudragit®
L 30D
Eudragit®
FS 30D
Eudragit®
L100-55
PVAP
HPMCP
HPMCP 50
HPMCP 55
CAP
6.0
7.0
5.6
6.8
5.5
5.0
4.5-4.8
5.2
5.4
5.0
PVAP = Polyvinyl acetate phthalate; HPMCP = Hydroxy propyl methyl cellulose
phthalate; CAP= Cellulose acetate phthalate.
pH Dependent (or Delayed Release) Systems:
Solid formulations for colonic delivery that are based on pH-dependent drug release
mechanism are similar to conventional enteric-coated formulations but they differ in
target site for delivery and therefore type of enteric polymers. In contrast to conventional
enteric-coated formulations, colonic formulations are designed to deliver drugs to the
distal (terminal) ileum and colon, and utilize enteric polymers that have relatively higher
threshold pH for dissolution. Most commonly used polymers are derivatives of acrylic
acid and cellulose. These polymers have ability to withstand an environment ranging
from low pH (1.2) to neutral pH (7.5) for several hours. Apparently, it is highly desirable
for pH-dependent colonic formulations to maintain their physical and chemical integrity
9.
during passage throughthe stomach and small intestine and reach the large intestine
where the coat should disintegrate to release the drug locally. It should be however noted
that GI fluids might pass through the coat while the dosage form transits through the
small intestine. This could lead to premature drug release in the upper parts of GI tract
and as a result loss of therapeutic efficacy may occur. One approach to overcome this
problem is to apply higher coating levels of enteric polymers; however, this also allows
influx of GI fluids through the coat, and the thicker coats often rupture under the
influence of contractile activity in the stomach. In general, the amount of coating required
depends upon the solubility characteristics (solubility, dose/solubility ratio) of the drug,
desired release profile and surface area of the formulation, and composition of the coating
solution/dispersion.
Coating approach is one of the simplest formulation technologies available for
colon-specific delivery. It also offers significant advantage in terms of cost and ease of
manufacture. From formulation standpoint, coated dosage forms may be either single-unit
system or a multi-particulate system, and each of these may be a single-layer product or a
multi-layer product. In case of single-layered products, the coating may be composed of a
single enteric polymer that has a pH-dependent solubility or a mixture of two polymers
one of which is pH-dependent while other is pH independent.
Coating of pharmaceutical dosage forms:
Coating is done normally to ensure these
Protecting the drug from its surrounding environment (particularly air, moisture
and light) with a view to improve stability.
Modifying drug release, as in enteric coated, repeat action and sustained release
products.
Reducing the risk of interaction between incompatible components.
Masking unpleasant taste and odor.
Increasing the ease of administration.
10.
Pharmaceutical coating processes:
Basicallythere are five major techniques for applying coatings to pharmaceutical
solid dosage forms:
1. Sugar coating
2. Film coating
3. Enteric coating
4. Fluid bed or suspension coating
5. Compression coating
Present formulation involves seal coating of the tablet dosage form (drug being moisture
sensitive) and then enteric coating the same as it is to be protected in the stomach from
degradation, which makes the formulation delayed release. Hence the detailed
explanation is given on film- coating and enteric- coating methods.
Film Coating of Solid Dosage Forms:
Film coating is a process that involves the deposition of thin but uniform, polymer film
onto the surface of the core tablet. Unlike sugar coating, the flexibility afforded in film
coating allows additional substrates, other than just compressed tablets, to be considered
for coating (e.g. powder, granules, nonpareils, capsules). Coatings are applied
continuously to moving bed of material usually by means of a spraying technique,
although manual application procedures have been used. Historically, film coating was
introduced in the early 1950 to combat the shortcomings of the then predominant
sugarcoating process. Film coating has proved successful as a result of the many
advantages offered which includes,
Minimal weight increase (typical 2 to 3% of tablet core weight)
Significant reduction in processing times
Increased process efficiency and output
Increased flexibility in formulation
Improved resistance to chipping of the coating
Cost effectiveness
Acceptable for diabetic patients
11.
Enteric Coated Tablets:
Theenteric-coated tablets deliver the drug almost locally at a predetermined rate and for
a specified period of time with in the intestinal tract.
The purpose of delayed release is to protect a drug destroying by acidic pH particularly
those drugs which are acid labile for example omeprazole, pantoprazole, Rabeprazole
sodium etc. Enteric coatings are used either to protect a substance from degradation by
gastric fluids or to reduce stomach destructions caused by irrigational drugs. Tablets and
capsules specially coated to remain intact in the stomach and to yield their ingredients in
the intestine are termed as enteric coated. After contact with intestinal fluids, the coatings
swell independent of pH and release the active ingredients by a diffusion-controlled
mechanism.
Enteric Coating:
An enteric coating is a barrier applied to oral medication that controls the location in the
GIT region, where it is absorbed. Enteric refers to the small intestine, therefore enteric
coatings will dissolve in intestine and prevent release of medication before it reaches
small intestine and give desired pharmacological action. The prime intension is to delay
the release of drugs which were inactivated by the stomach contents or may cause nausea
or bleeding by irritation of gastric mucosa.
Coating is deposition of thin film of polymer surrounding the tablet core. Conventional
pan equipments may be used but now-a-days more sophisticated equipments are
employed to have a high degree of automation and quality coating. The polymer is
solubilised in solvent & other additives like plasticizers and pigments are added.
Resulting solution is sprayed onto a rotated tablet bed. The drying conditions cause
removal of the solvent, giving thin deposition of coating material around each tablet.
12.
Significance of Entericcoating:
To protect acid-labile drugs from the gastric fluid.
To protect from gastric distress or nausea due to irritation of the drug.
To deliver drugs intended for local action in the intestine.
To deliver drug that are optimally absorbed in the small intestine to their primary
absorption site in their most concentrated form.
To provide a delayed release component to repeat actions.
Protect the drugs from harmful effect of the gastric contents because some of the
drugs are prone to be hydrolyzed in acid media (Eg: Rabeprazole sodium, Esomeprazole,
Omeprazole, Pantaprazole).
Enteric Coating Polymers:
Enteric coatings are usually formulated with synthetic polymers that contain ionizable
functional groups that render the polymer water soluble at a pH value. Since many of
these enteric polymers are esters, they may be subject to degradation (as a result of
hydrolysis) when exposed to conditions of elevated temperature and humidity; such
hydrolysis can result in a substantial change in enteric properties.
Properties of an Ideal enteric coating polymer:
1. Resistance to gastric fluids.
2. Ready susceptibility to or permeability to intestinal fluids.
3. Compatibility with most coating solution components and the drug substrates.
4. The film should not change on aging.
5. Formation of continuous film.
6. Non-toxicity.
7. Low cost.
8. Ease of application
13.
A polymer withthreshold pH in the range of 5 to 6 is considered ideal for an
enteric coat. This is based on the premises that the pH of the stomach, even in the fed
state, will rarely reach this level but will exceed duodenum, where secretion of
bicarbonate neutralizes the acidic chyme leaving the stomach. There is no single polymer
that applicable for the enteric coating all drug molecules. The nature of core materials
(acidity, basicity or permeability through different enteric polymer films) may limit the
choice of polymer.
Cracking of the film either during application or on storage will result in a loss of enteric
properties. Therefore, consideration must be given to the mechanical properties of the
applied film. Cracking problems can be effectively overcome by plasticization.
Plasticizer can also be used to reduce the permeability of the polymer films to water
vapor. The choice of suitable plasticizer is restricted to non-water soluble materials
because these are likely to be most effective.
General rule to follow is to use 1 part plasticizer to 10 parts polymer. One should also
considered viscosity of the plasticizer, its influence on the final coating solution, its effect
on film permeability, tackiness, flexibility, solubility, taste, toxicity, compatibility with
other coating solution components, stability of the film and the final coated product.
Most enteric coatings won't dissolve in solutions with a pH lower than 5.5.
Commonly-used enteric coating polymers:
1. Methacrylic acid copolymers.
2. Cellulose acetate (and its succinate and phthalate version).
3. Polymethacrylic acid/acrylic acid copolymer.
4. Hydroxy propyl methyl cellulose phthalate.
5. Polyvinyl acetate phthalate.
6. Hydroxy ethyl ethyl cellulose phthalate.
7. Cellulose acetate tetrahydrophtalate.
8. Acrylic resin.
9. Shellac.
14.
Cellulose AcetatePhthalate (CAP)
It is an effective enteric coating which dissolves above pH 6. It is permeable to
moisture and simulated gastric fluid in comparison with other enteric polymers and it is
susceptible to hydrolytic breakdown on storage.
Poly Vinyl Acetate Phthalate (PVAP)
Less permeable to moisture and simulated gastric juice, it is more stable to hydrolysis
on storage. Enteric dosage forms coated with PVAP disintegrates at pH 5.
Hydroxy Propyl Methyl Cellulose Phthalate (HPMCP)
It is available in two grades HP50 and HP55.
HP55 solutions are more viscous than HP50.
HP50 disintegrates at pH5 and HP55 disintegrates at pH5.5.
It has stability similar to that of PVAP and dissolves in the same pH range. The
advantage is that it does not require plasticizer.
Methacrylic acid copolymers
Two grades are available A and B which differs in the ratio of free carboxyl to ester
groups therefore,
Type A has a ratio of 1:1 and disintegrates at pH 6.
Type B has a ratio of 1:2 and disintegrates at pH 7.
The earliest enteric coatings utilized formalized gelatin, this was unreliable because of
the polymerization of gelatin could not be accurately controlled. Another was shellac;
disadvantage was polymerization with time, resulting in poor dissolution of the coating.
The most extensively used polymers are CAP, PVAP and recently used polymers are
HPMC phthalate, Methacrylic acid copolymers.
15.
Other additives:
Plasticizer:
The qualityof coating can be modified by the use of plasticizers. Plasticizers
can modify the physical and chemical properties of the polymers. Optimization of
plasticizer must be concentration based on presence of other additives. Some of the
commonly used plasticizers are castor oil, propylene glycol, Di acetylated
monoglycerides, polysorbates and organic acid esters.
Colorants:
Colorants are used to provide distinctive color and elegance to a dosage form. To
achieve proper distribution of suspended colorants in the coating solutions requires the
use of fine powdered colorants. The most common colorants in use are certified food
drug and cosmetics colorants. These are synthetic dyes or lakes of dyes.
Solvents:
The primary function of a solvent system is to dissolve or disperse the polymers
and other additives and convey them to the substrate surface. The most widely used
solvents for enteric coating polymers are water, ethanol, methanol, isopropanol,
chloroform, acetone etc.