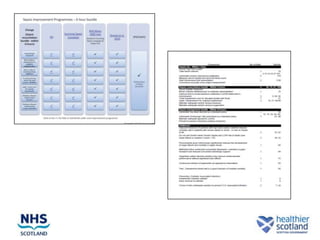
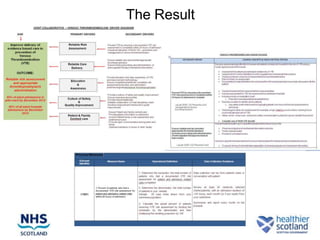
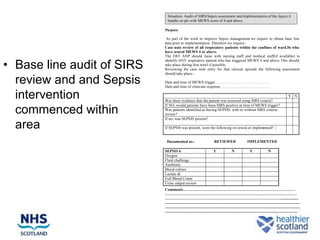
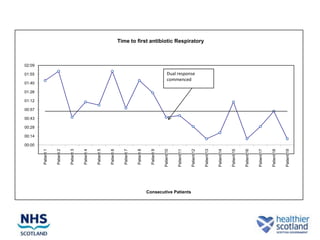
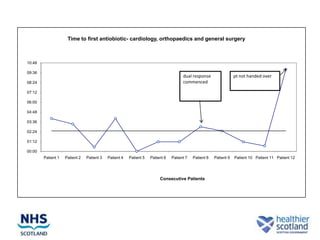
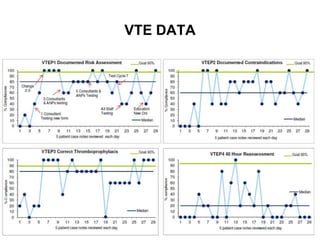
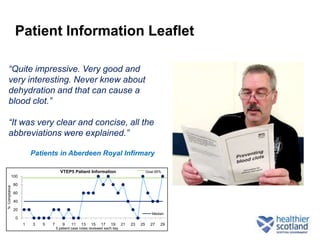
The document discusses the Sepsis/VTE Collaborative. It explains that the collaborative was formed to improve sepsis and venous thromboembolism (VTE) management. It describes initial tests of changing documentation and assessing patients for sepsis that were conducted. Baseline data was collected on 18 patients with high early warning scores, of which 9 had new septic episodes. The median time to first antibiotics for septic patients was reduced from 1 hour and 25 minutes pre-intervention to 37 minutes post-intervention with the introduction of a dual response system in one respiratory ward area. Balancing measures such as antibiotic usage were also tracked.