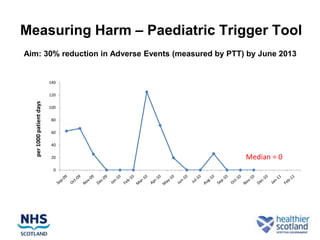
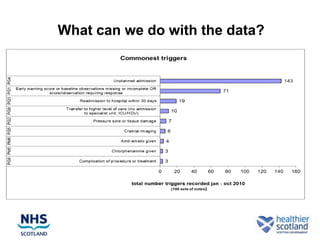
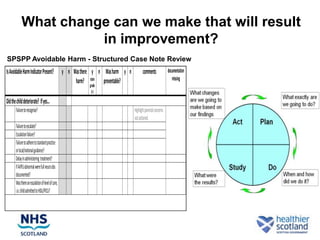
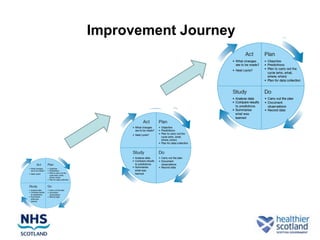
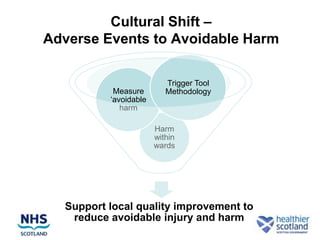
The document summarizes the Scottish Patient Safety Paediatric Programme (SPSPP), which aims to reduce adverse events in pediatric hospital care in Scotland by 30% by June 2013. The SPSPP uses a pediatric trigger tool to measure adverse events and identify areas for improvement. It takes a multidisciplinary approach including subject matter experts to conduct reviews of cases involving potential adverse events or avoidable harm. The goal is to test changes and improvements that address common causes of harm or system failures, and track metrics to know if the changes are leading to lower rates of avoidable harm.