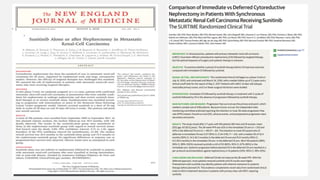
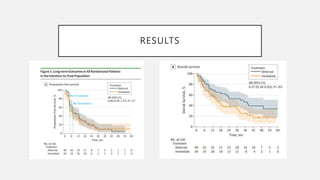
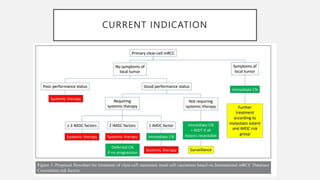
The document discusses the role and implications of cytoreductive nephrectomy (CN) in metastatic renal cell carcinoma (RCC), highlighting its historical importance and evolving nature of treatment paradigms influenced by advancements in systemic therapies. Benefits of CN include alleviation of symptoms and potential enhancement of immune responses, while disadvantages encompass increased morbidity and delays in systemic treatment initiation. Recent clinical trials suggest that while CN may offer survival benefits in certain patient subsets, deferred approaches and the introduction of immunotherapies warrant further evaluation of its efficacy.


































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)




