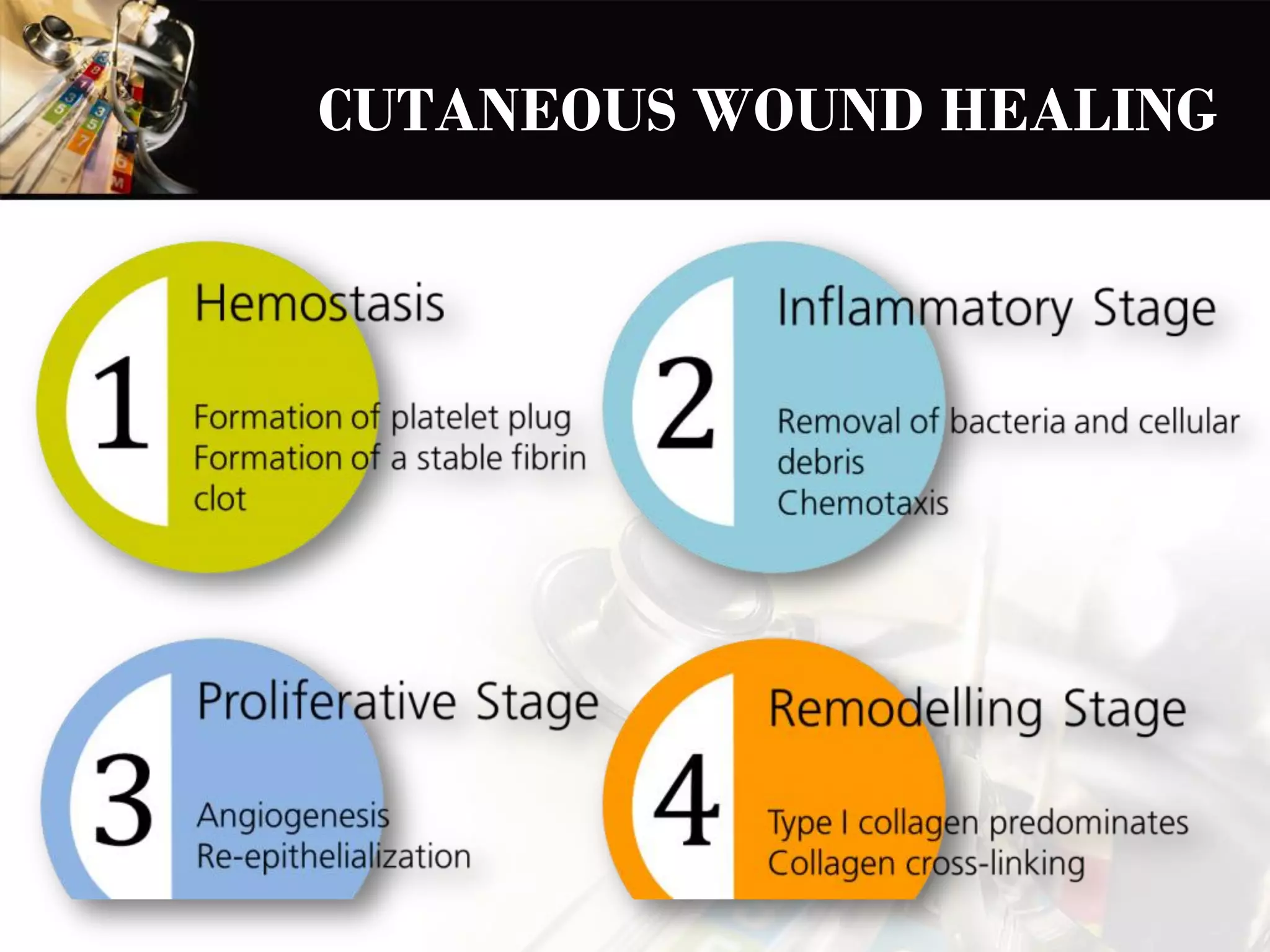
Cutaneous wound healing occurs through first or second intention. Primary union (first intention) involves clean surgical incisions approximated by sutures, resulting in relatively thin scar formation. Secondary union (second intention) involves larger defects without sutures, resulting in formation of granulation tissue and more substantial scarring due to wound contraction. The stages of wound healing include formation of a blood clot, granulation tissue, re-epithelialization, collagen deposition, and scar formation.