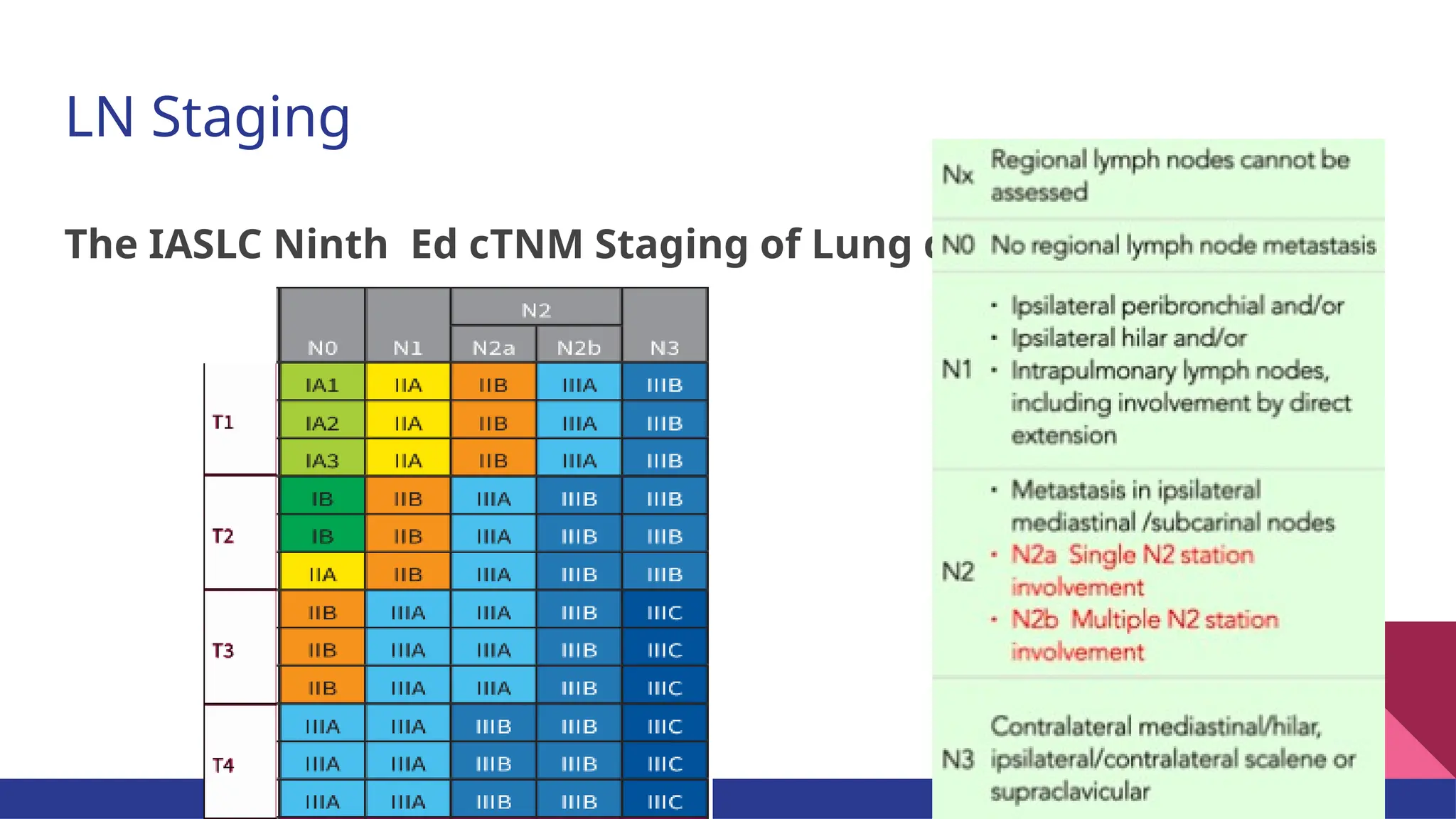
Mediastinal dissection for lung cancer is one of the controversial but a cross-cutting surgical management aspect of lung cancer. This presentation, which is based on the 9th ed. of TNM staging of lung cancer and associated IASCLC update on lymph node mapping, gives a good summary of the up-to-date approach to investigate the node status of lung ca. More importantly, it brings together the summary of the literature on the spearhead studies done to compare mediastinal lymph node dissection to systematic sampling.