Downloaded 49 times


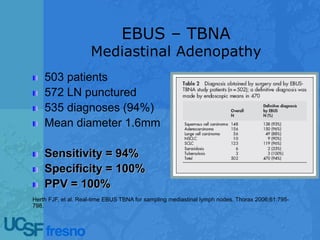
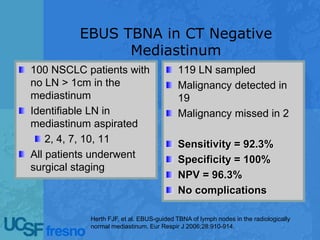
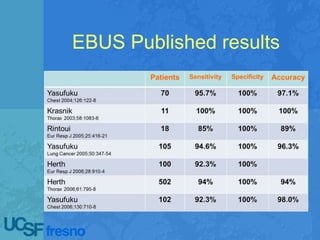
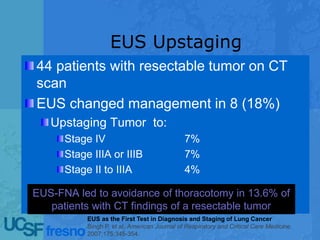
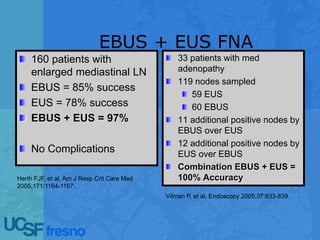
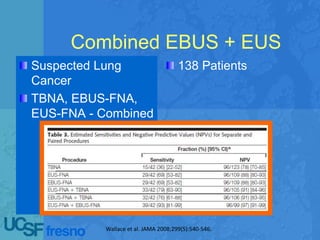




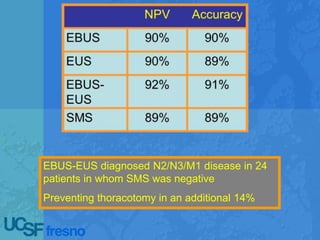








Echoendoscopic lymph node staging in lung cancer provides an endoscopic alternative to surgical staging that is minimally invasive, accurate, and prevents unnecessary surgeries. Combined endobronchial ultrasound and endoscopic ultrasound (EBUS/EUS) procedures sample lymph nodes and detect metastasis with a sensitivity of 91% and specificity of 96%, outperforming surgical staging. EBUS/EUS is now considered the new gold standard for mediastinal staging as it is safer, less costly, and more comprehensive than surgical staging alone.