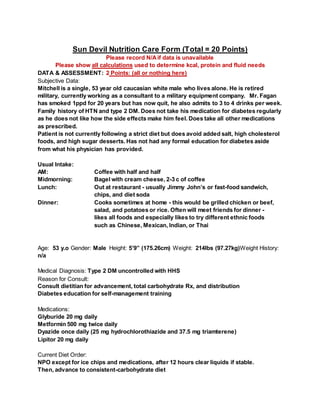
Mitch, a 53-year-old man with uncontrolled type 2 diabetes, was admitted to the ER with hyperglycemic hyperosmolar syndrome (HHS). His blood glucose was 1524 mg/dL and osmolality was 360 mmol/kg/water. He was started on insulin therapy with Lispro and glargine to control his blood sugar. As his diabetes was poorly controlled for an extended period, he is at high risk for chronic complications and will likely need to continue insulin. The nutrition consult will focus on diabetes self-management education and transitioning Mitch to a consistent carbohydrate diet.