

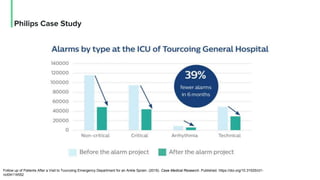
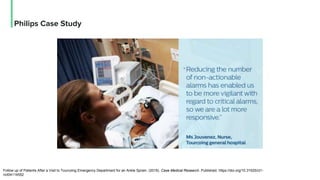
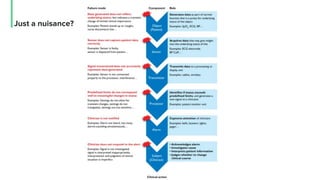
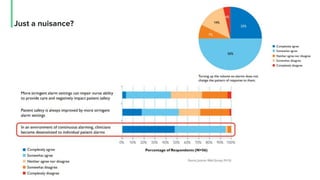

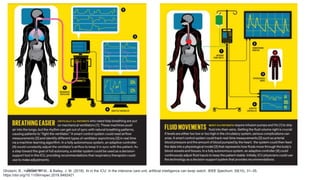


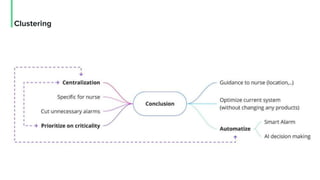
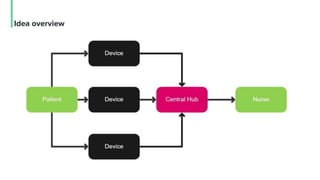

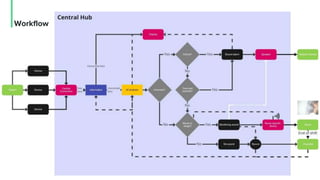
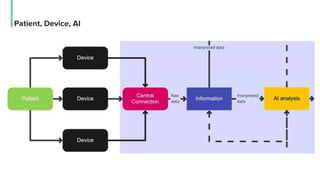
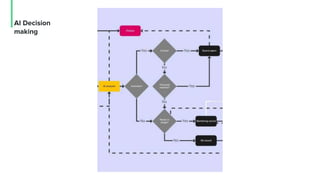
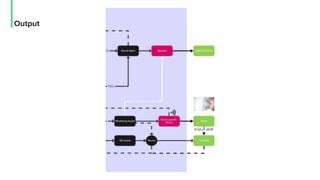
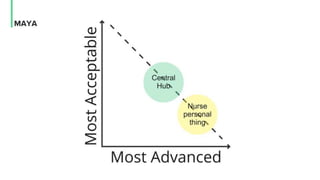
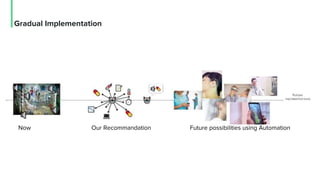
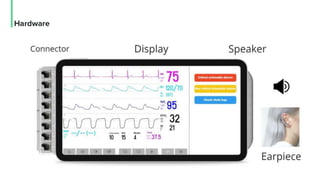
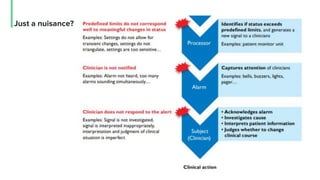
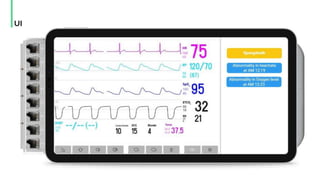
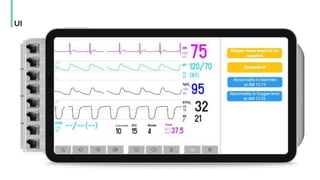
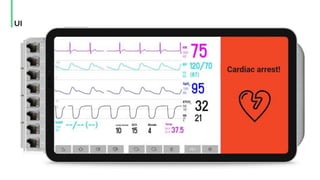
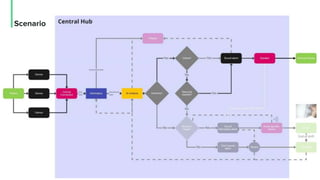

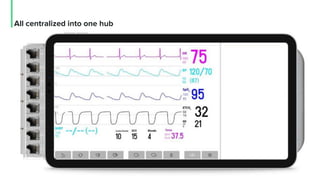


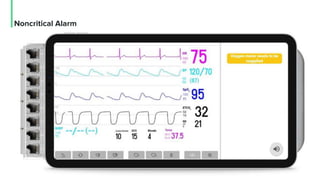

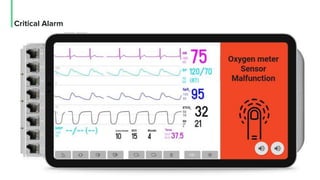


The document discusses the management and optimization of alarm systems in the ICU to mitigate alarm fatigue and improve patient care. It proposes using AI to prioritize alarms and modify their sounds based on criticality levels, suggesting a centralized hub for alarms linked to patient devices. The conclusions emphasize the importance of balancing critical and non-critical alarms to enhance the responsiveness of medical staff.









































































