Downloaded 95 times
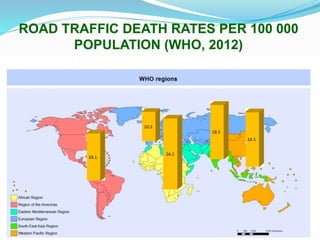
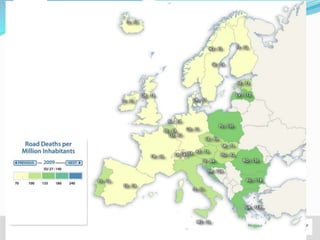
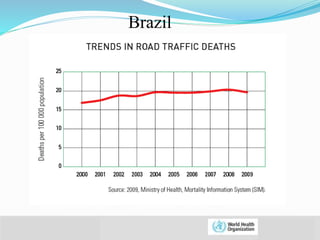
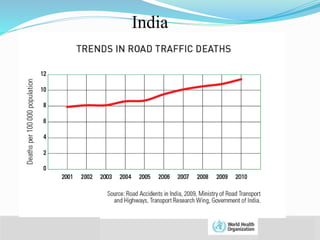
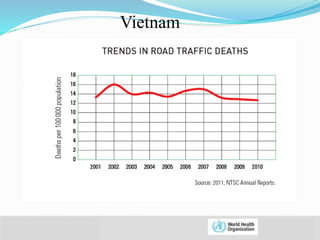
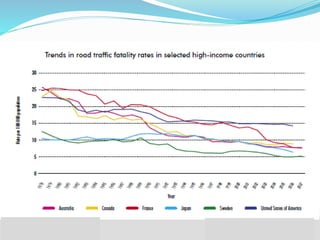
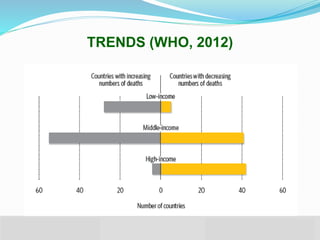
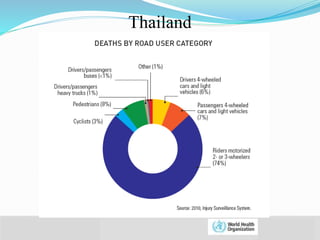
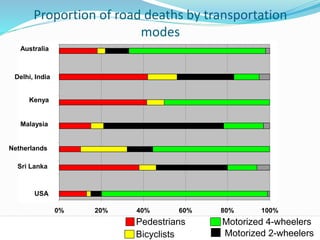
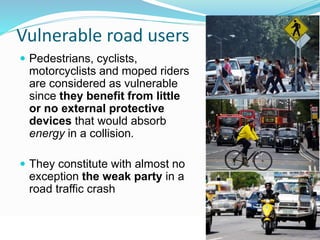
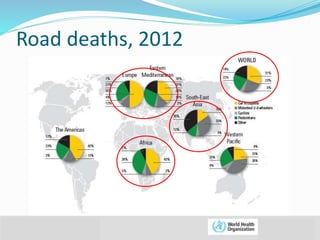
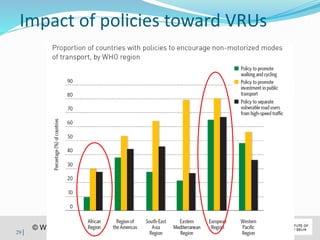
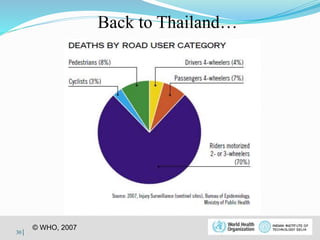


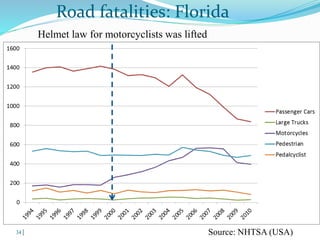
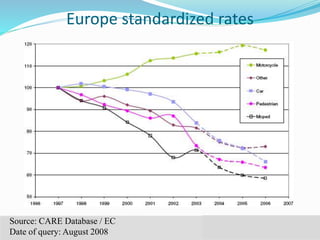















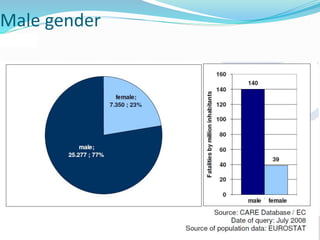
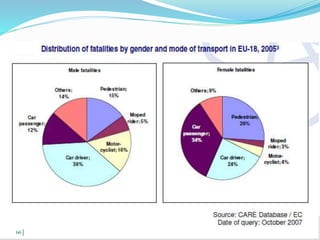
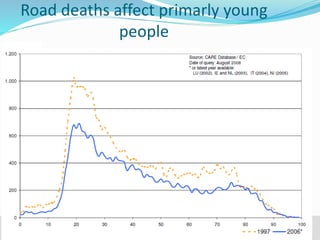
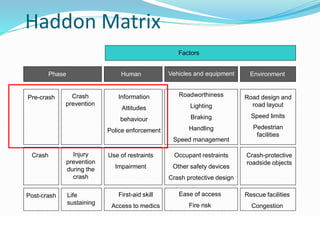
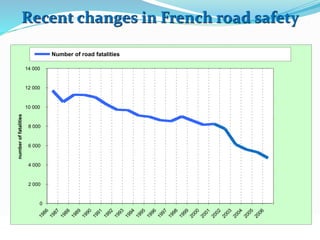


Road traffic crashes are a major public health issue that cause over 1 million deaths per year globally. Vulnerable road users such as pedestrians, cyclists and motorcyclists account for about half of road traffic deaths. Factors that influence the risk of road traffic injuries include human behaviors like speeding, driving under the influence of alcohol, and lack of safety measures like helmet and seatbelt use. Policies and infrastructure changes that enhance road safety, especially for vulnerable users, have been shown to significantly reduce road traffic fatalities.







































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)














