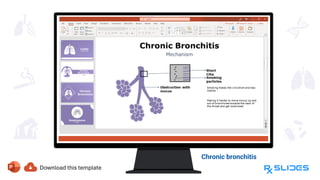
Chronic Obstructive Pulmonary Disease (COPD) encompasses progressive lung diseases like chronic bronchitis and emphysema, leading to airflow obstruction and breathing difficulties. Major risk factors include smoking, air pollution, and genetic predispositions, with specific stages of the disease correlating to symptom severity. Treatment options focus on bronchodilators, anti-inflammatory medications, and lifestyle changes to improve respiratory function and quality of life.