Downloaded 25 times

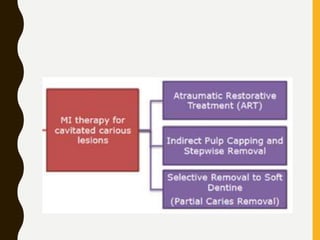

This document discusses conservative strategies for managing dental caries, including mechanical, chemico-mechanical, and physical approaches. Mechanical approaches include ART, indirect pulp capping, stepwise excavation, and selective removal to soft dentine. Chemico-mechanical caries removal uses chemical agents to soften infected dentin before excavation. Physical approaches include photodynamic antimicrobial chemotherapy, which uses photosensitizing agents activated by light to kill bacteria. The document compares the pros and cons of these different conservative caries management techniques.