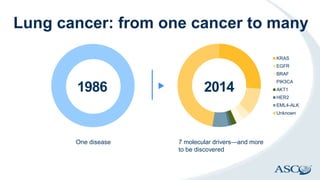
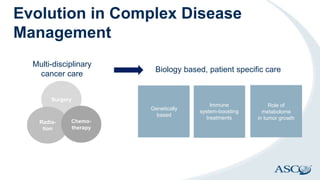
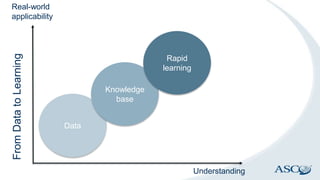
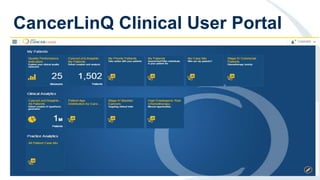
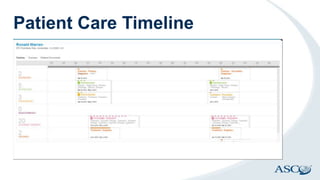
CancerLinQ aims to harness big data to improve cancer care by learning from every patient. It faces challenges of integrating diverse data types from genomics to behaviors. Its goals are precision, personalized medicine through molecular profiling of individual cancers. As clinical trials enroll few patients, CancerLinQ would provide real-world data from electronic health records to uncover new insights. When deployed, it will analyze de-identified patient records to uncover care patterns, allow comparing care to guidelines and peers, and provide evidence-based guidance. This has the potential to improve outcomes for patients and quality for providers and researchers.