Introduction
CKD isa worldwide public health problem, both
for the number of patients and cost involved.
With growing age of the population prevelence
is increasing.
Lack of knowledge to screen early and also to
manage them rightly increasing morbidity and
mortality among CKD patients.
4.
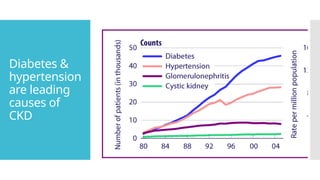
Magnitude
of the
burden
• Thereported prevalence of CKD in different
regions of India ranges from <1% to 17%(ISN
2018).
• Over 50% of patients with advanced CKD are
first seen when the eGFR is <15 ml/min per 1.73
m2
.
• This sobering number highlights the need for
robust screening programs for those at risk for
CKD
5.
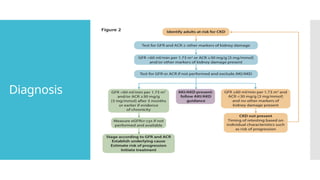
Diagnosis
Chronic kidneydisease (CKD) is defined
as either structural or functional
impairment of the kidney for three or
more months, irrespective of the
cause.
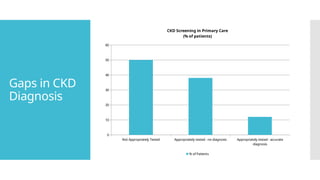
Gaps in CKD
Diagnosis
NotAppropriately Tested Appropriately tested - no diagnosis Appropriately tested - accurate
diagnosis
0
10
20
30
40
50
60
CKD Screening in Primary Care
(% of patients)
% of Patients
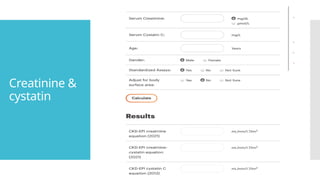
Creatinine
& cystatin
Noideal marker yet
We have only functional marker no structural
markers.
No troponin or AST for kidney
Both of them are late markers
Hence rapid action is required once elevated.
Serial values are important to know the rate of fall
of GFR
eGFR calculation – CKDEPI is preferred ( 2012)
What’s new – cystatin in the formula
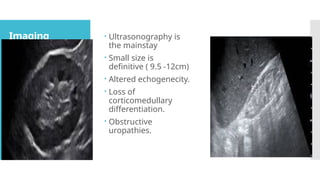
Imaging Ultrasonographyis
the mainstay
Small size is
definitive ( 9.5 -12cm)
Altered echogenecity.
Loss of
corticomedullary
differentiation.
Obstructive
uropathies.
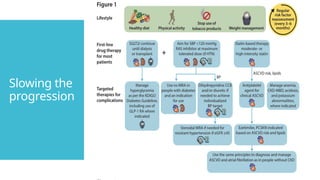
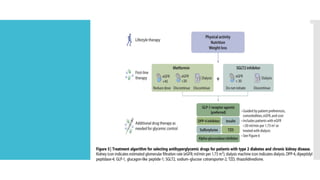
Managemen
t
Treatment ofreversible causes of kidney failure
Preventing or slowing the progression of kidney
disease
Treatment of the complications of kidney
failure .
Adjusting drug doses when appropriate for the
level of estimated glomerular filtration rate
(eGFR).
Identification and adequate preparation of the
patient in whom kidney replacement therapy
will be required
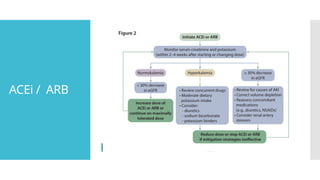
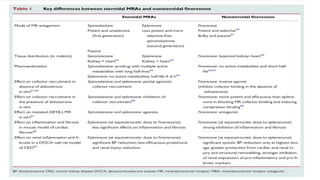
Finerenone
The
Forgotten ‘A’
of RAAS
string
Finerenone is a non-steroidal third generation Mineralocorticoid
receptor antagonist.
It has high affinity for the Mineralocorticoid receptor does not bind
to androgen receptor
It reduces albuminuria
It improves cardiovascular outcomes and also renal outcomes
Two major studies FIDELIO DKD and FIGARO DKD have shown
significant improvement with respect to RENAL &
CARDIOVASCULAR outcomes
There is an increased risk of hyperkalaemia
Use in combination with SGLT2 inhibitors requires further study
31.
Too early not
justearly .
Protective therapy has the greatest impact if it is initiated
before the plasma creatinine concentration exceeds 1.2 -
1.5 mg/dL
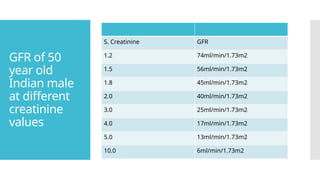
32.
GFR of 50
yearold
Indian male
at different
creatinine
values
S. Creatinine GFR
1.2 74ml/min/1.73m2
1.5 56ml/min/1.73m2
1.8 45ml/min/1.73m2
2.0 40ml/min/1.73m2
3.0 25ml/min/1.73m2
4.0 17ml/min/1.73m2
5.0 13ml/min/1.73m2
10.0 6ml/min/1.73m2
Complication
s
Metabolic acidosis
ImprovesGrowth in
children
Delays progression
of CKD
Preserves bone
health
Reduces
inflammation
Prevents cachexia
Target above 22
meql/dl
Caution about
volume expansion
Hyperkalemia
DIET & DRUGS
Food leaching
RAASi ,MRA, Beta
blockers,NSAIDS.
Minimise with
diuretics and alkali
therapy
35.
ANEMIA
Worsens cardiacfailure , frequent
hospitalisation, repeated transfusion, infections,
sensitisation
Relative deficiency of Erythropoietin and abnormal
hypoxia sensing mechanism .
Correct the iron ,B12, frolic acid deficiency.
ESA – Erythropoetin, darbopetin, peqylated rHu
EPO
DUSTATS ( HIF STABILIZERS - desidustat,
vadadustat, roxadustat,molidustat,daprodustat)
36.
CKD MBD
Triard
Osteodystrophy, vascular calicification , high
phosphate ,low calcium, high
pth(paratharmone).
Spectrum – a Dynamic bone disease to renal
osteodystrophy
Treatment - Correct vit D deficiency,
hypocalcemia , hyperphosphatemia ( dietary
restriction, oral phosphate binders, calcitriol,
calcimmetics)
37.
Dyslipidemia
Mainly hypertriglycerdemiawith total
cholesterol being normal.
Screen all patients with CKD
In DM, Nephrotic syndrome , metabolic
syndrome may have elevated cholesterol ,
treatment is with statins and ezetimibe.
Secondary prevention is similar to non CKD
patients
Primary prevention-
1. All patients with GFR <60ml/min
2. Patients with CKD and GFR >60ml/min and
age>50yrs or other risk factors.
38.
Malnutrition
Protein diet.? Need customisation For Indian
patients
ICMR (2020) – 0.6gm/kg body weight.
Restrict in glomerular disease in early stage.
Restrict animal protein.
Calorie - 30 to 35kcal /kg / day
39.
Infection and
vaccination
Higherrisk of infections compared to general
population
Vaccination :
Influenza – annual.
Hepatitis B – 4 doses ( double dose)
Pneumococcal ( prevenar 13 & pneumovac 23)
40.
Medications
in CKD
CKDpatients at high risk for drug-related adverse events
•Several classes of drugs renally eliminated
•Consider kidney function and current eGFR (not just SCr)
when prescribing meds
•Minimize pill burden as much as possible
•Remind CKD patients to avoid NSAIDs
•No Dual RAAS blockade
•Any med with >30% renal clearance probably needs dose
adjustment for CKD
•No bisphosphonates for eGFR <30
•Avoid GAD for eGFR <30
41.
Referral to
Nephrologist
s
When
GFR< 30 ml/min/1.73m2.
Earlier in whom GFR is falling rapidly and with
albuminuric CKD
Rapid fall - >5ml/min/1.73m2/ year .
Why
To Plan and counsel about renal replacement therapy
Access(vascular & peritoneal Dialysis)
To counsel about renal transplantation
42.
Referral to
Nephrologist
s
latereferral is associated with a significantly
increased risk of all-cause mortality.
Early referral enables discussion of the
preferred mode of kidney replacement therapy
to suit the patient's lifestyle.
Helps in timely placement of a permanent
dialysis access.
Patients treated by nephrologists were
significantly less likely to have required a
temporary venous catheter for the first dialysis
(36 versus 89 percent).
Kidney
replacement
therapy
Hemodialysis (incentre / home )
Peritoneal dialysis ( intermittent/ continuous)
Kidney transplantation – treatment of choice,
as it improves quality of life and reduces
mortality.
45.
Hemodialysi
s
Pros
Widely available
Under government schemes
Less patient involvement .
Regular monitoring by Nephrologists
Cons
Thrice a week ( care giver fatigue)
Not a continuous process(unphysiological)
hemodynamic unstability
Access issues.- Fistula first catheter kills
Painful
46.
Peritoneal
dialysis
Pros
Homebased
Patient involved in his own care
More independent.
More physiological and liberal food intake
Less BP variations.
Cons
Abdominal discomfort.
Peritonitis.
Lack of Patient smartness.
Less effective once patient is Anuric
47.
Kidney
transplantati
on
Treatment ofchoice
As it replaces all the functions of the kidney.
Live related / deceased donor(JSK).
Swap transplantation program.
Abo incompatible transplants.
Cons.
Cost
Availability of the kidney
Stigma in society (Donor and receipent)
Immunosuppression risk for the recipient
Graft loss ( rejection, recurrence of basic disease)
48.
Take home
Robustscreening of high risk patients for early diagnosis .
Lifestyle modifications are equally important as pills.
Use of Disease modifying drugs and regular monitoring.
Timely referral to Nephrologists
Preparing for kidney replacement therapy
Encourage deceased donor and swap transplantation.
#4 Increases risk for all-cause mortality, CV mortality, kidney failure (ESRD), and other adverse outcomes.
#10 Use of cystatin c along with creatnine strengthens the association between the eGFR and risk of death.
Muscle mass
All nucleated cells ( obesity smoking crp )
Epidemiology collaboration equation