This document summarizes a quality improvement project aimed at enhancing and sustaining authentic hourly visitation (AHV) to improve patient outcomes and experience. Methodologies used included a SWOT analysis, interviews, questionnaires, literature review, PDSA cycles, and chart reviews. Barriers to consistent AHV identified through staff questionnaires included time constraints, inadequate staffing, patient conditions, and interruptions. The project recommendations are to maintain collaboration between leadership and staff, ongoing data collection and review, and for leadership to address staff needs and challenges.
PowerPoint: Practical Approaches to Improving Patient Pre-Op PreparationEmCare
Michael Hicks, MD, MBA, FACHE, CEO of EmCare Anesthesia, and Lisa Kerich, PA-C, VP of Operations for EmCare Anesthesia, provide expert advice for improving the performance of your O.R. through an integrated, collaborative approach. Learn how Pre-Anesthesia Testing (PAT) clinics are being used successfully to improve patient readiness, surgeon satisfaction and financial performance.
Originally presented Sept. 17, 2015, as a webinar in partnership with Becker's Hospital Review.
In this presentation from the Beryl Institute's 2016 Patient Experience Conference, Edwards-Elmhurst Healthcare’s ED Chair and Patient Experience Director detail how they are leveraging technology to follow up with ED Patients and the exceptional results they’ve enjoyed.
How one Hospital Shaved Off 88 Minutes from their ALOSEmCare
With goals of getting the right processes and staffing in place, the administration and staff at LewisGale Medical Center in Salem, Virginia put a priority on patient-centered process improvements that would shorten wait times and length of stay in the emergency department (E.D.). Here’s how they improved metrics including decreasing the ED ALOS by 45 percent.
PowerPoint: Practical Approaches to Improving Patient Pre-Op PreparationEmCare
Michael Hicks, MD, MBA, FACHE, CEO of EmCare Anesthesia, and Lisa Kerich, PA-C, VP of Operations for EmCare Anesthesia, provide expert advice for improving the performance of your O.R. through an integrated, collaborative approach. Learn how Pre-Anesthesia Testing (PAT) clinics are being used successfully to improve patient readiness, surgeon satisfaction and financial performance.
Originally presented Sept. 17, 2015, as a webinar in partnership with Becker's Hospital Review.
In this presentation from the Beryl Institute's 2016 Patient Experience Conference, Edwards-Elmhurst Healthcare’s ED Chair and Patient Experience Director detail how they are leveraging technology to follow up with ED Patients and the exceptional results they’ve enjoyed.
How one Hospital Shaved Off 88 Minutes from their ALOSEmCare
With goals of getting the right processes and staffing in place, the administration and staff at LewisGale Medical Center in Salem, Virginia put a priority on patient-centered process improvements that would shorten wait times and length of stay in the emergency department (E.D.). Here’s how they improved metrics including decreasing the ED ALOS by 45 percent.
This resource summarizes the eight recommendations outlined in the Institute of Medicine's a new consensus study entitled, Improving Diagnosis in Health Care. The recommendations are aimed at making diagnoses more accurate, reliable, efficient, and safe. This work is a continuation of the IOM’s Quality Chasm series.
Annette Bartley: Making it happen - Intentional RoundingThe King's Fund
Annette Bartley, Independent Healthcare Consultant, The Health Foundation, highlights the key findings of the CQC report on the State of Care and discusses the benefits of Intentional Rounding for patients.
Presented at the George Washington University 1st GME Retreat. Includes overview of handoff function and content, pitfalls for handoffs, and strategies for safe and effective communication during handoffs, and how to use process improvement techniques to make handoffs safer. Handout includes handoff menu of educational tools to be used by faculty teaching.
In 2011, we took it upon ourselves to break down our patient care and examine it from the time the patient arrived (regardless of method) to the time they departed (again, regardless of method). Over the next year, we developed and implemented an end-to-end strategy of patient care and flow, where all decisions were under the scrutiny of what was deemed to be ‘patient-centric’. This process of self-improvement led us to develop a scalable, replicable template for hospitals of all shapes and sizes. Too often, patient flow hurdles and patient care problems are addressed solely through the vantage of individual departments at the expense of efficiency. Our presentation is the result of a personal, real-time experience.
Quality management in nursing professionSANJAY SIR
Quality improvement requires in any field to provide best services to the community in the health care system. it is uploaded to aware the the paramedics & nursing personnel to improve the quality care & helps educators to teach their students.
What can a Clinical Nurse Leader do for your critical care nursing unit? Plenty! Consider this new nursing role as one that can improve patient outcomes and increase satisfaction for both clients and staff. Successful microsystems begin with empowering patients, families and front line nurses.
An Orientation to quality and patient safety for new hire in health care faci...kiran
An introduction to quality and patient safety for new employees in health care with basic concepts on quality and patient safety that every new hire must know.
Tricks of the Trade: Patient Recruitment & Retention for Different Study TypesImperial CRS
In efforts to raise the bar for medical advancement, clinical trials are growing increasingly complex. This complexity, more often than not, leads to costly delays in enrollment. In this ebook, we'll take a look at 4 case studies for different study types, and examine the unique factors to consider during planning.
This resource summarizes the eight recommendations outlined in the Institute of Medicine's a new consensus study entitled, Improving Diagnosis in Health Care. The recommendations are aimed at making diagnoses more accurate, reliable, efficient, and safe. This work is a continuation of the IOM’s Quality Chasm series.
Annette Bartley: Making it happen - Intentional RoundingThe King's Fund
Annette Bartley, Independent Healthcare Consultant, The Health Foundation, highlights the key findings of the CQC report on the State of Care and discusses the benefits of Intentional Rounding for patients.
Presented at the George Washington University 1st GME Retreat. Includes overview of handoff function and content, pitfalls for handoffs, and strategies for safe and effective communication during handoffs, and how to use process improvement techniques to make handoffs safer. Handout includes handoff menu of educational tools to be used by faculty teaching.
In 2011, we took it upon ourselves to break down our patient care and examine it from the time the patient arrived (regardless of method) to the time they departed (again, regardless of method). Over the next year, we developed and implemented an end-to-end strategy of patient care and flow, where all decisions were under the scrutiny of what was deemed to be ‘patient-centric’. This process of self-improvement led us to develop a scalable, replicable template for hospitals of all shapes and sizes. Too often, patient flow hurdles and patient care problems are addressed solely through the vantage of individual departments at the expense of efficiency. Our presentation is the result of a personal, real-time experience.
Quality management in nursing professionSANJAY SIR
Quality improvement requires in any field to provide best services to the community in the health care system. it is uploaded to aware the the paramedics & nursing personnel to improve the quality care & helps educators to teach their students.
What can a Clinical Nurse Leader do for your critical care nursing unit? Plenty! Consider this new nursing role as one that can improve patient outcomes and increase satisfaction for both clients and staff. Successful microsystems begin with empowering patients, families and front line nurses.
An Orientation to quality and patient safety for new hire in health care faci...kiran
An introduction to quality and patient safety for new employees in health care with basic concepts on quality and patient safety that every new hire must know.
Tricks of the Trade: Patient Recruitment & Retention for Different Study TypesImperial CRS
In efforts to raise the bar for medical advancement, clinical trials are growing increasingly complex. This complexity, more often than not, leads to costly delays in enrollment. In this ebook, we'll take a look at 4 case studies for different study types, and examine the unique factors to consider during planning.
Quality and safety, Vision 2025, Specific challenges of Nursing on quality, Quality improvement division, Fish bone technique,QI model, PDCA, Role of Nurse, Empowerment, Nursing positioning and policies,
HFMA Article: 5 Signs That You Can Reduce Staffing Costs and Boost Nurse Sati...Block & Tackle Marketing
See how three Care Logistics hospitals are increasing efficiency in care delivery to improve healthcare quality and nurse morale while reducing costs from overtime, agency use, and turnover. By Care Logistics CFO Samantha Platzke.
Ward Handover enables a more efficient handover of patients between shifts enabling a more effective patient discharge process. The solution is split into two parts, based around 6PM's CareSolutions database:
Ward Handover System:
A proven ward handover application which enables clinical staff to maximize their care time whilst delivering a single view of the patient by allowing them to enter the discharge notes into a single location that may be accessed by all clinical teams involved in the patient's care – including doctors, ward nurses, specialist nurses and Allied health Professionals. The system therefore allows predictability of bed utilization to maximize their occupancy and assists the bed management team in proactive assessment whilst reducing overall costs of related activities.
Patient Discharge Reporting:
The second part of the solution is real time reporting. The solution takes feeds from the Trust's CRS application every 15 minutes regarding patient status and predicted discharge dates which is then used to create a number of reports for ward staff regarding the workload and patient status. These reports can then be viewed either by ward staff or by consultants.
Is
su
e
B
r
Ie
f
C AL I FORNIA
HEALTHCARE
FOUNDATION
June 2010
Workflow Redesign:
A Model for California Clinics
Introduction
Patient flow, particularly initial patient access
and cycle time, is crucial to community clinic
practice efficiency and capacity, which in
turn affects revenue and provider and patient
satisfaction.1 As a clinic improves patient access,
it increases the timeliness of patient care, and
thus may improve outcomes, and in some cases
the odds that a patient will receive care at all.
Balancing appointment supply and demand, and
establishing and managing provider panels, can
increase access and improve practice efficiency
and patient satisfaction. Moreover, effective
panels and resulting continuity can strengthen
prevention efforts, improve outcomes for patients
with diseases that can be detected early, and
help manage chronic conditions through regular
monitoring.
Improved access and practice efficiency, and
resulting clinical improvement, depend on
factors specific to each clinic — such as goals
and priorities, physician preferences, and
patient population — which together constitute
a particular practice system. While there
are many approaches a clinic might take to
address individual aspects of practice efficiency,
meaningful practice redesign requires a thorough
understanding of the practice’s patient care
processes and identification of practice-specific
strategies for improving efficiency. Such practice
redesign requires a multi-component approach,
which can be enabled and enhanced by the
application of a comprehensive, field-tested
framework for change.
In 2007, the California Primary Care Association
(CPCA), funded by the federal Bureau of Primary
Health Care and facilitated by Mark Murray and
Associates, launched the Optimizing Primary
Care Collaborative (OPCC) as a one-year learning
project. The collaborative, with 21 community
clinic teams, was designed to reduce patient
flow delays in primary care settings and to
improve clinical care. Following the first year’s
work, in 2008 the same partners organized a
second OPCC, with additional funding from
the California HealthCare Foundation (CHCF).
A total of 24 community health clinics from
California and Arizona participated in the
2008 OPCC. The collaborative used a learning
community framework to help clinic teams set
goals, collect data, and measure effects.
Upon completion of OPCC in 2009, CHCF
supported an evaluation of its methods and
outcomes by White Mountain Research Associates
(White Mountain). The evaluation found that the
level of improvement varied among clinic sites, but
that there was marked overall success: Virtually all
participants saw improvements, with 88 percent
of teams reporting positive changes in at least
two access and patient satisfaction measures,
and 63 percent reporting positive changes in
three or more of these m.
Strategies of addressing unwarranted variation in wound care
Chukwu Poster
1. Enhancing and sustaining Authentic
Hourly Visitation to Improve Outcome
and Care Experience
Nneka Christiana Chukwu MSN, RN, CNL
METHODOLOGIES
• Strength, Weaknesses, Opportunities, and Threats (SWOT) analysis
• Informational interview
• Questionnaires
• Literature review
• PDSA
• Chart review
• SWOT ANALYSIS
RECOMMENDATIONS
• Maintain consistent collaboration between the leadership team
and the front-line staff to preserve the AHV process.
• Ongoing collection and review of data to ensure sustainability.
• Need for leadership team to listen and respond to the needs
and challenges identified by staff.
SELECTIVE REFERENCES
Daniels, J.F. (2016). Purposeful and timely nursing rounds: a best
practice implementation project. Joanna Briggs system reviews and
implementation reports. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/26878929
Kaiser Permanente. (n.d.). Authentic hourly visitation for nurses: an
evidence-based practice for performance improvement. Retrieved
from www.kp.org.
Stanford Health Care. (n.d.). Nursing quality and safety: purposeful
rounding. Retrieved from
https://stanfordhealthcare.org/health-care-professionals/nursing/qu
ality- safety/purposeful-rounding.html
ACKNOWLEDGEMENT
My sincere gratitude goes to my Director Josephine Reyes for all her
support.
I offer my heartfelt thanks to my teachers Dr. Cathy Coleman and
Nancy Taquino for their selfless efforts and learning opportunities.
Finally, to my parents and children, my deepest appreciation and
acknowledgment.
ABSTRACT
Authentic hourly visitation (AHV) otherwise known as purposeful
rounding or hourly rounding is an evidence-based process, which
focuses on safety of hospitalized patients using a proactive
approach. Regular and purposeful, proactive rounding promotes
safety, comfort, and responsiveness which has a direct impact on
the care experienced by patients and their satisfaction with service
delivery. The setting for this improvement project was the medical
surgical unit and medical telemetry unit at Kaiser South San
Francisco. This process improvement project aims to enhance and
sustain the frequency and quality of Authentic Hourly Visitation.
Improving the frequency and consistency of this interactive
practice will ensure that patients receive timely and efficient care
with a resultant improvement in their care experience. This goal is
in alignment with that of this integrated delivery health care
organization, which thrives to provide the highest quality of care to
every patient at all, times. The CNL as an outcomes manager, risk
anticipator and educator led this process improvement project in
collaboration with all key players in these microsystems by
administering questionnaires, informational interviews, chart
review and observation.
Keywords: Authentic hourly visitation, barriers, care experience,
patient safety, care experience.
NURSING IMPLICATIONS
Nurses are charged with providing safe and efficient care to
patients. This is critical especially at a time when healthcare is
undergoing reformation (value based purchasing). Healthcare
institutions are no longer reimbursed for hospital acquired
conditions or provision of sub-standard care. Additionally, the
Centers for Medicare and Medicaid Services fine organizations for
never events such as falls and hospital acquired pressure ulcers.
This places financial burden on the organization. Furthermore,
following implementation of Affordable Care Act (ACA) -
Obama-care, patients are no longer limited to one healthcare plan.
The implication is that patients who are not satisfied with their
level of care can transfer care to another provider. Clearly,
identifying and resolving barriers to AHV can impact the ultimate
improvement in outcome of patient care as well as team and
patient engagement.
TIMELINE
OBJECTIVES
To identify and eliminate barriers to Authentic Hourly Visitation.
To increase the overall rating of the hospital from 68.3% to 80% by
December 2016.
To improve the quality and frequency of AHV in order to make it
more meaningful to staff and patients.
SIGNIFICANCE
• Performing the 4PS (presence, pain, position, & potty) during
AHV improves outcome of care and overall HCAHPS scores.
• AHV decreases the use of call light among hospitalized patients,
decreases fall rate, and decreases interruptions in the workflow
of the nurses and patient care technicians
LITERATURE REVIEW
The study of Daniel (2016) on hourly rounding showed a 5%
increase in nurse to patient communication and an 11% increase in
pain management scores. He cited the Institute for Healthcare
Improvement (IHI) who “endorsed hourly rounding as the best way
to reduce call lights and fall injuries, and increase both quality of
care and patient satisfaction” (p.1).
Similarly, Stanford Health Care published the result of a research
conducted in 14 hospitals on hourly rounding which showed that
hourly rounding led to 14% decline in pressure ulcers and 12%
increase in patient satisfaction scores. One of the hospitals
reported a 20% decline in the distance the nurses walk each shift.
5/25 6/3-
6/12
8/95/27 6/13-
6/21
6/23 6/28-
7/11
7/12-
7/19
7/20
8/5
Identify and define project
topic
Aim Statement & Background
Develop Charter and
Questionnaire. Meeting with
professor Coleman for update
Review of literature and
questionnaire
Review and update project
charter and questionnaires
Microsystem assessment with
manager.
Work on charter
Meeting with IT for data
collection
Hand out questionnaires to
staff for data collection
Data analysis and updates
Putting it all together. Review
of project and presentation to
preceptor and other leaders.
Final poster Presentation
• Decrease patient falls and hospital
acquired pressure ulcers
• Improve nurse to patient communication
• Decrease use of call lights
• Improve patient care experience
• Increase HCAHPS scores
• Cost savings for the organization
• Improvement in patient satisfaction
scores.
• Changes in the rounding process
(provide chairs for nurses to sit in the
patients’ rooms) to make it more efficient.
• Staff have received training on AHV
• CNL in the microsystem will lead the
process in collaboration with frontline
staff.
• Addressing barriers to AHV
• Creating a location for staff to
document AHV
Strengths Weaknesses
Opportunities Threats
• Inconsistent rounding by nursing staff.
• Rounding that is not meaningful
• Interruptions during rounding
• Lack of team collaboration and frontline
staff participation in decision making
process
• Lack of follow up
• Inadequate staffing
• Reimbursement
• Loss of clientele to competitors
• Loss of reimbursement dollars
MODEL FOR IMPROVEMENT
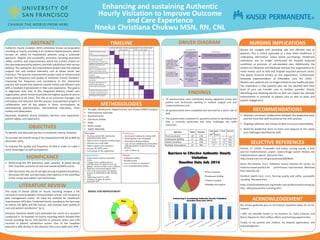
FINDINGS
• 70 questionnaires were distributed among registered nurses and
patient care technicians working in medical surgical unit and
medical telemetry unit.
• 60 questionnaires were completed and returned for a return rate of
90%
• The questionnaire contained 11 questions aimed at identifying how
AHV is currently performed and what challenges the staffs
encounter.
Barriers Total Percent
Time Constraint 10 17%
Inadequate Staffing 17 28%
Patient Condition 9 15%
Multiple Interruptions 24 40%
Total Percent
1-5 7 12%
5-10 35 58%
10-15 12 20%
>15 6 10%
Time Spent
on
AHV (mins)
DRIVER DIAGRAM