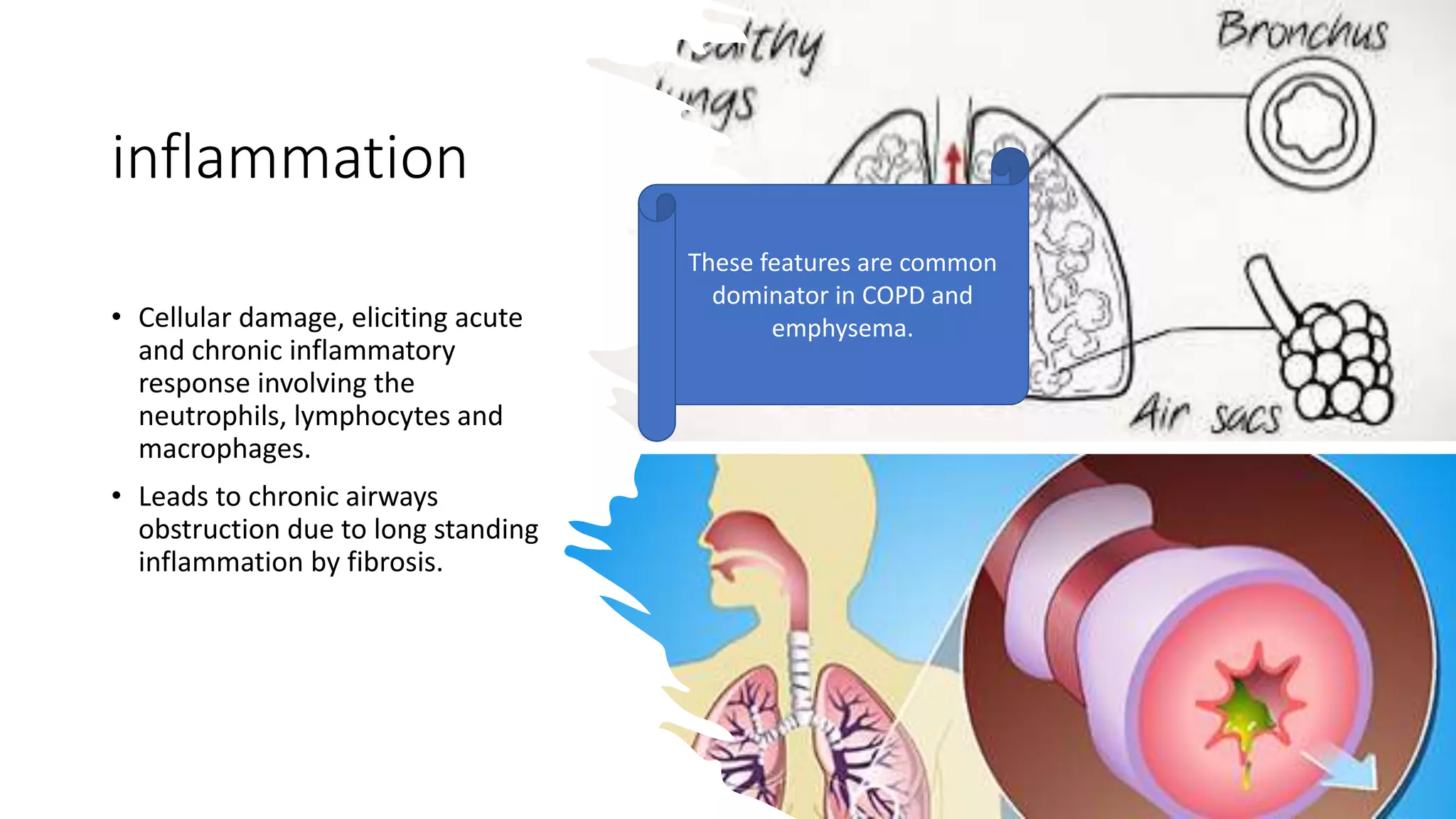
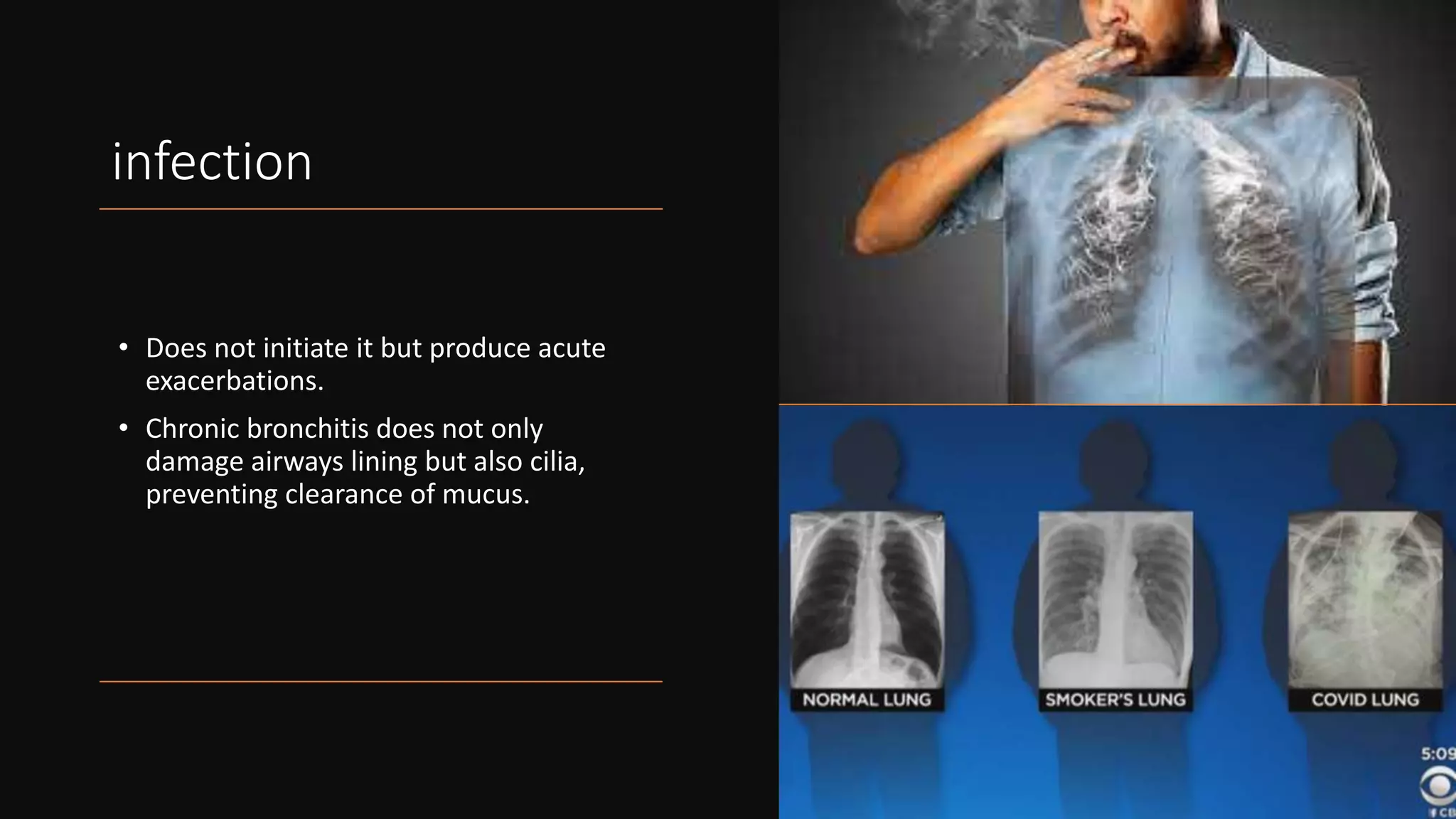
Chronic bronchitis is characterized by a decline in lung function, heart failure, and potential cancerous development due to dysplasia of the respiratory epithelium. It involves mucus hypersecretion in the large airways due to hypertrophy of submucosal glands and increased goblet cells. This causes chronic inflammation and long-term airway obstruction due to fibrosis. Infections do not initiate chronic bronchitis but can cause acute exacerbations by preventing mucus clearance. Changes in the mucous membrane include hyperemia, edema, hyperplasia and an increased Reid index. Clinical features include persistent cough, sputum, dyspnea, and potentially hypoxemia, cyanosis and cardiac failure over the