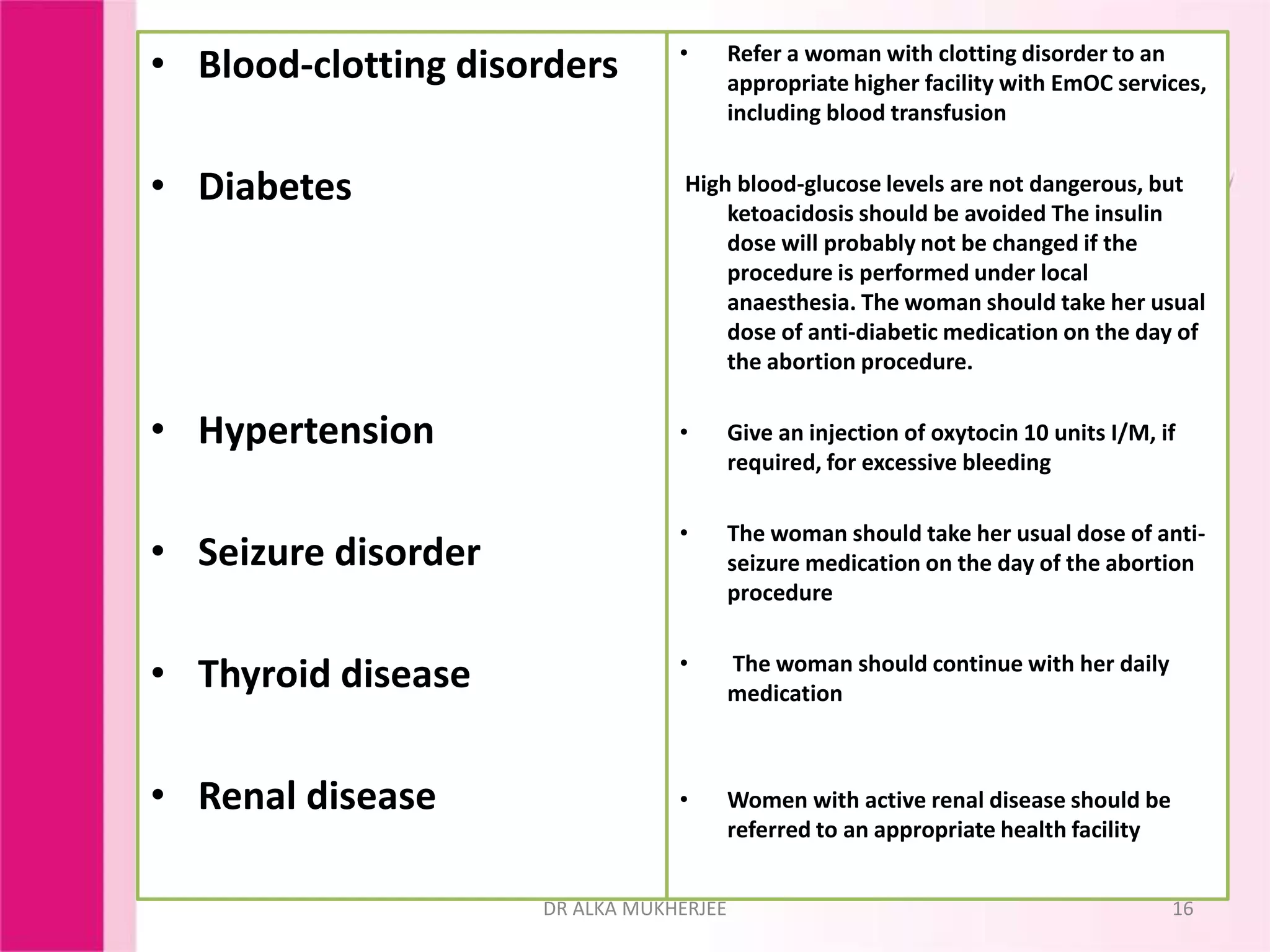
Dr. Alka Mukherjee provides a comprehensive clinical assessment framework for women seeking termination of pregnancy, emphasizing the importance of detailed history taking, physical and pelvic examinations, and necessary laboratory investigations. The document outlines critical components such as evaluating the woman’s health, gestational age, and any associated medical conditions that may complicate the procedure. It also stresses caution and the need for referral to specialized facilities when complications or higher-level care is required.





























































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)




