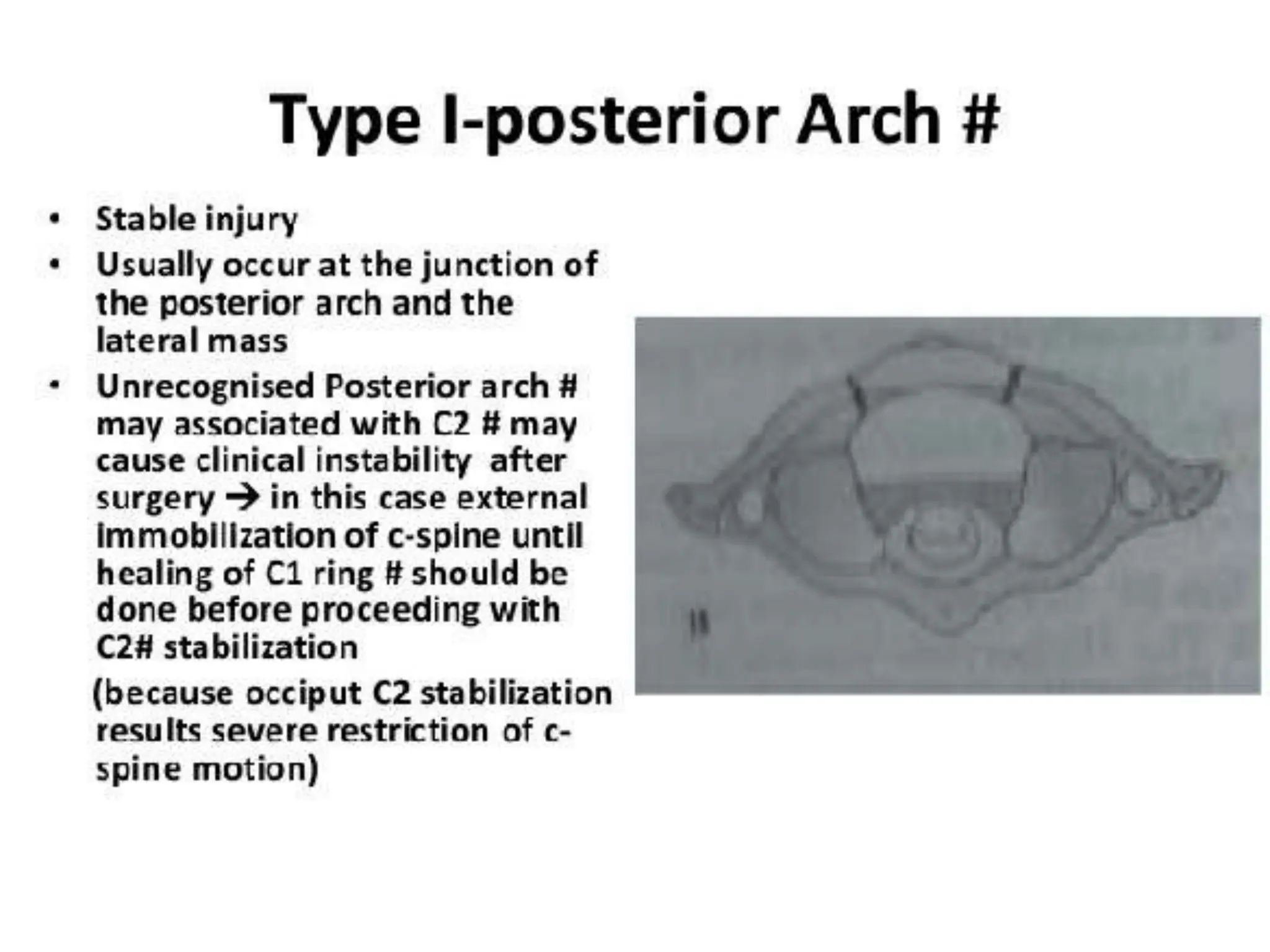
This document discusses fractures of the atlas (C1 vertebra). It notes that atlas fractures make up around 7% of cervical spine fractures and have a low risk of neurological injury. They are commonly missed on initial imaging due to the location at the occipitocervical junction. Mechanisms of injury include hyperextension, lateral compression, and axial compression. Around 50% have an associated spine fracture and 40% are associated with an axis (C2) fracture. Imaging such as CT is the preferred method to delineate fracture patterns and identify other cervical spine injuries. Conservative treatment with a hard collar or halo immobilization for 6-12 weeks is indicated for stable fractures with an intact transverse ligament. S