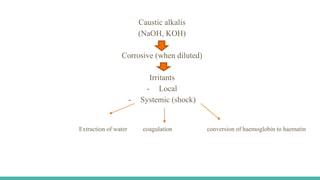
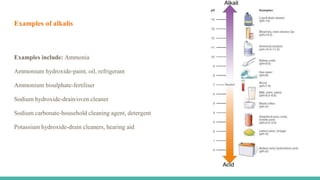
The document discusses alkali toxicity, focusing on caustic ingestions, which are more frequent in adults than children due to intentional ingestion. It outlines the epidemiology, exposure modes, symptoms, complications, diagnosis, and treatment options associated with alkali poisoning, highlighting the severe consequences of ingestion on the gastrointestinal tract and other body systems. The document emphasizes the importance of proper medical management and the potential long-term effects, including esophageal strictures and cancer.