Downloaded 36 times



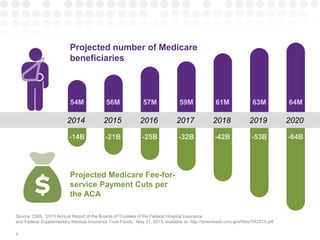
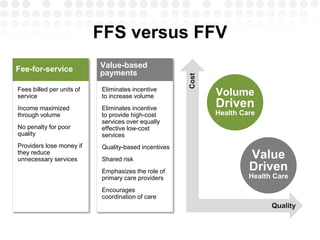


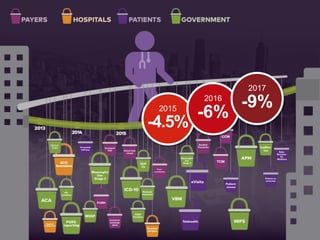
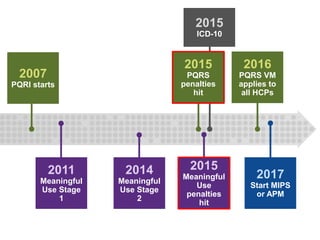


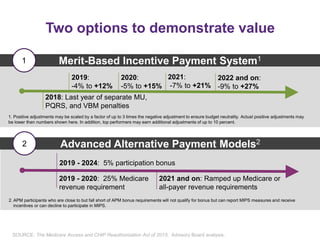

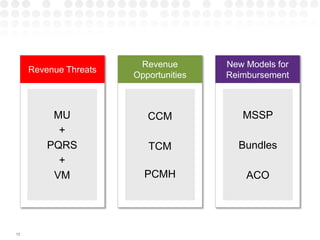
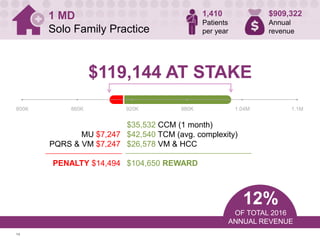
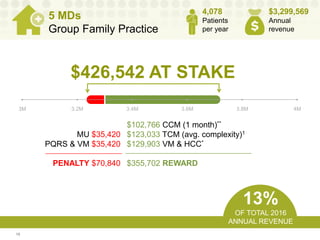
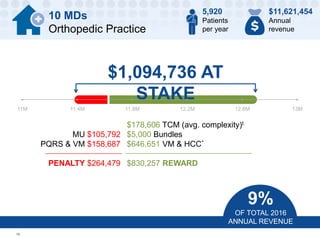
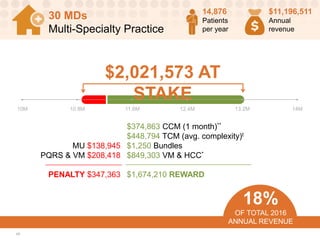

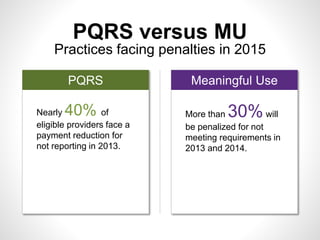


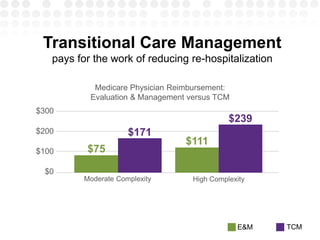












The document discusses projected Medicare fee-for-service payment cuts and emphasizes the shift from volume-driven to value-driven healthcare. It highlights the roles of various incentive programs and the financial stakes for different medical practices under the changes in reimbursement models. It also details the importance of coordinated care and quality-based payments, with statistics on Medicare beneficiaries and penalties for non-compliance with the established healthcare standards.























![Cuban American Medical Society Presentation[1]](https://cdn.slidesharecdn.com/ss_thumbnails/finalajkcubanamericanpresentation1-110126010033-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)






















































