Download to read offline


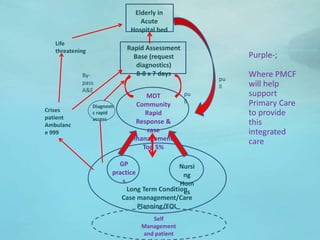


This document summarizes plans for collaboration between 10 GP practices in Darlington, England covering 94,000 patients. It discusses using funding from the Prime Minister's Challenge Fund (PMCF) to improve patient care through greater collaboration between primary care providers, the local Foundation Trust hospital, and the local council. Key goals include increasing flexibility and access to care, improving management of elderly patients, and evaluating options for expanded hours on weekends. Challenges mentioned include increasing patient demand, limited resources, change management difficulties, and addressing legal/data sharing issues when patients receive care from multiple providers. Support is requested in areas like communications, evaluation, and learning from other successful collaborations.























































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)