Can Endolaparoscopic Techniques Solve all surgical
1.
Can Endo LaparoscopicTechniques
Solve All Surgical Problems?
dr. Tommy Ruchimat, Sp.B, Subsp.BD(K)
1st
Beyond the Scalpel (B.t.S.)
Controversies in Trauma & Minimally Invasive Surgery
2.
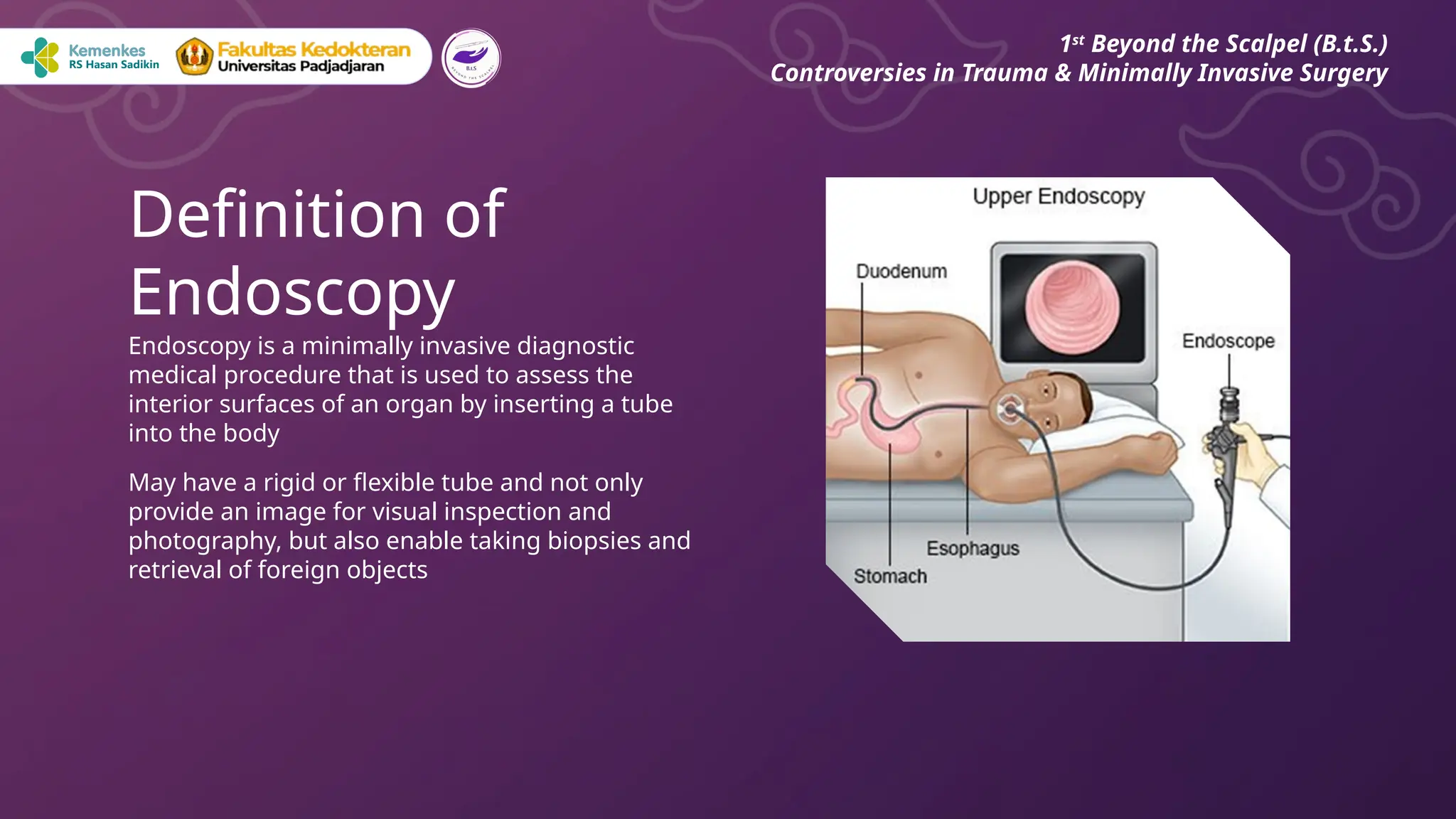
Endoscopy is aminimally invasive diagnostic
medical procedure that is used to assess the
interior surfaces of an organ by inserting a tube
into the body
May have a rigid or flexible tube and not only
provide an image for visual inspection and
photography, but also enable taking biopsies and
retrieval of foreign objects
Definition of
Endoscopy
1st
Beyond the Scalpel (B.t.S.)
Controversies in Trauma & Minimally Invasive Surgery
3.
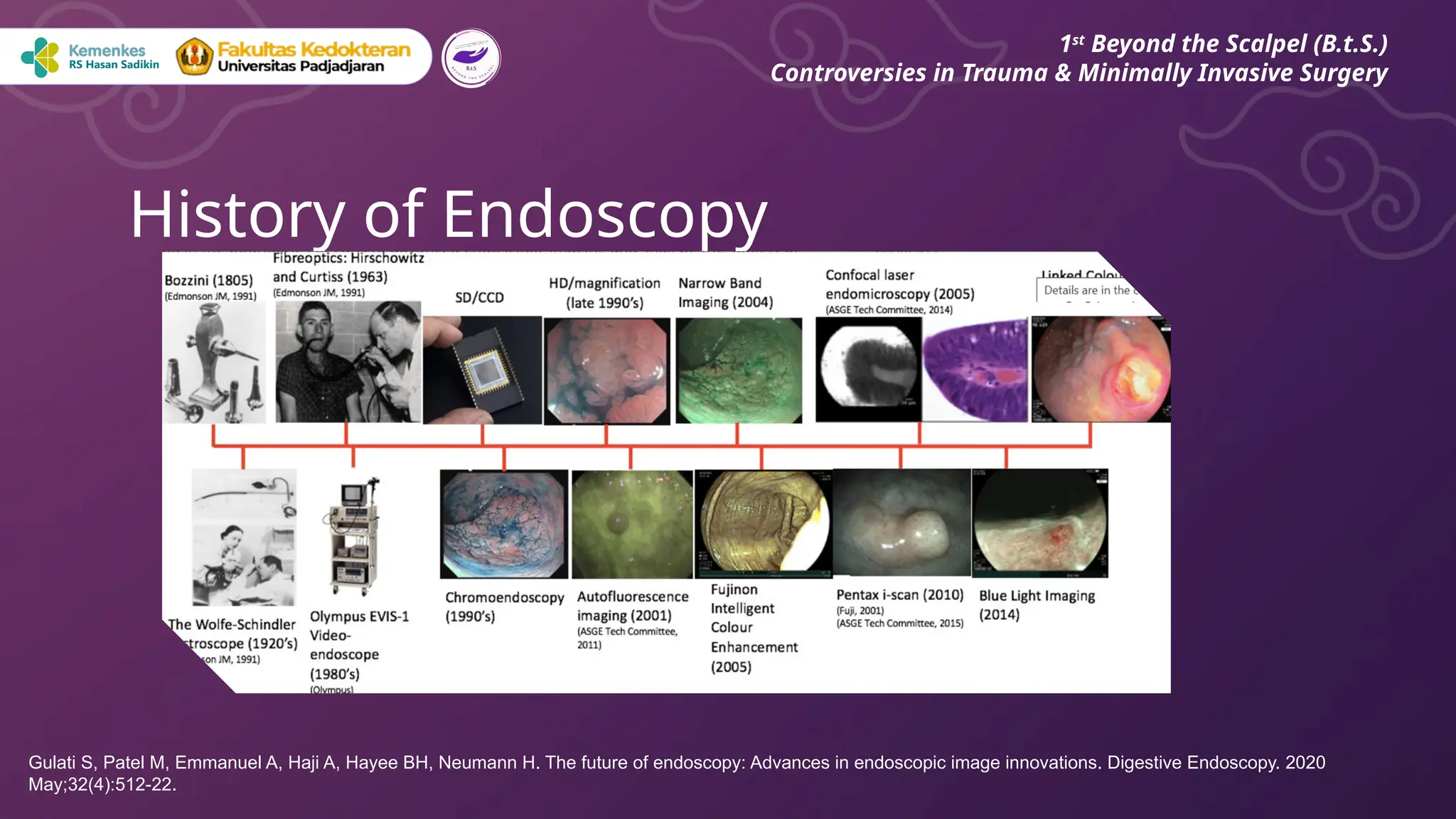
History of Endoscopy
1st
Beyondthe Scalpel (B.t.S.)
Controversies in Trauma & Minimally Invasive Surgery
Gulati S, Patel M, Emmanuel A, Haji A, Hayee BH, Neumann H. The future of endoscopy: Advances in endoscopic image innovations. Digestive Endoscopy. 2020
May;32(4):512-22.
4.
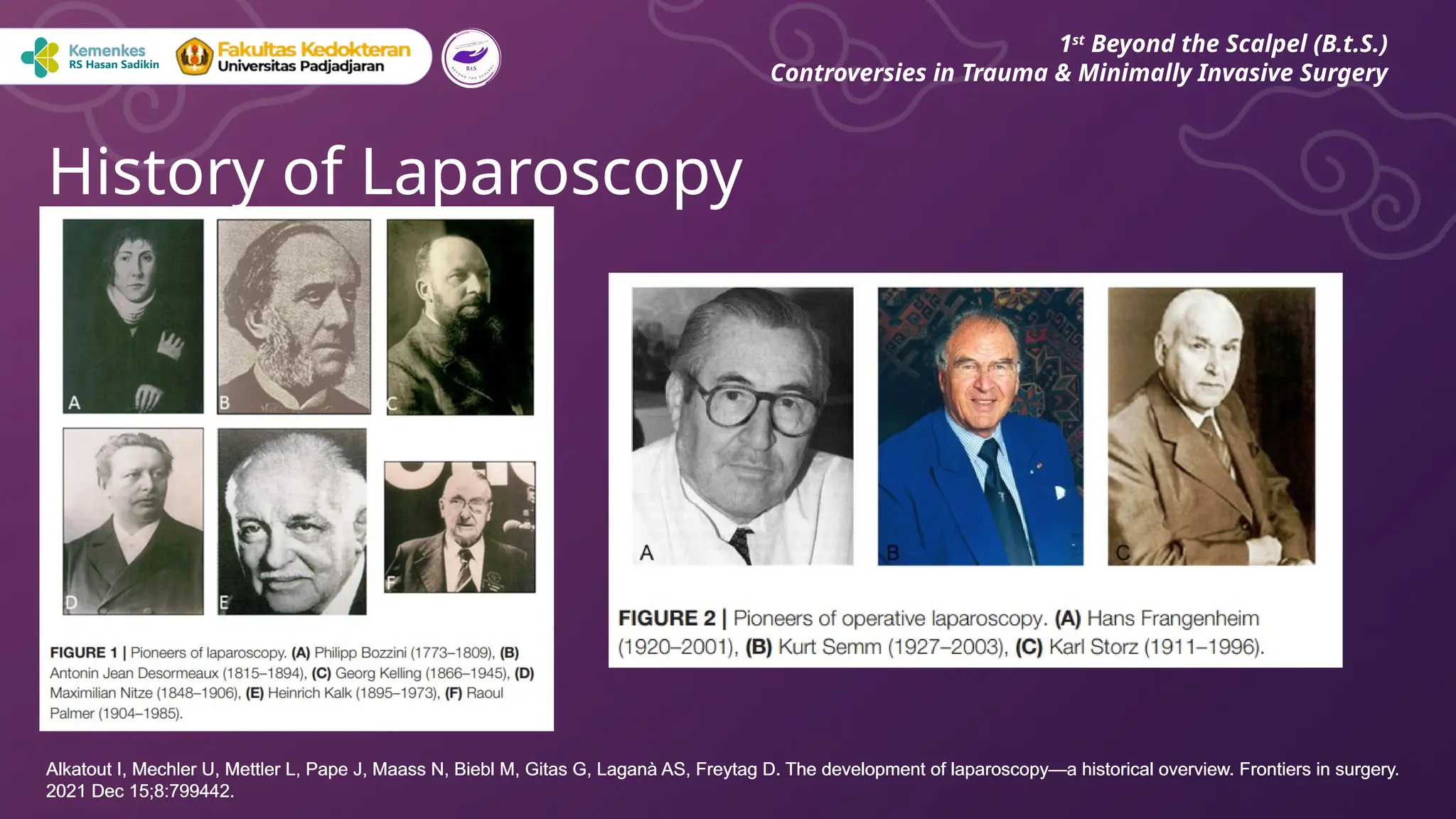
History of Laparoscopy
1st
Beyondthe Scalpel (B.t.S.)
Controversies in Trauma & Minimally Invasive Surgery
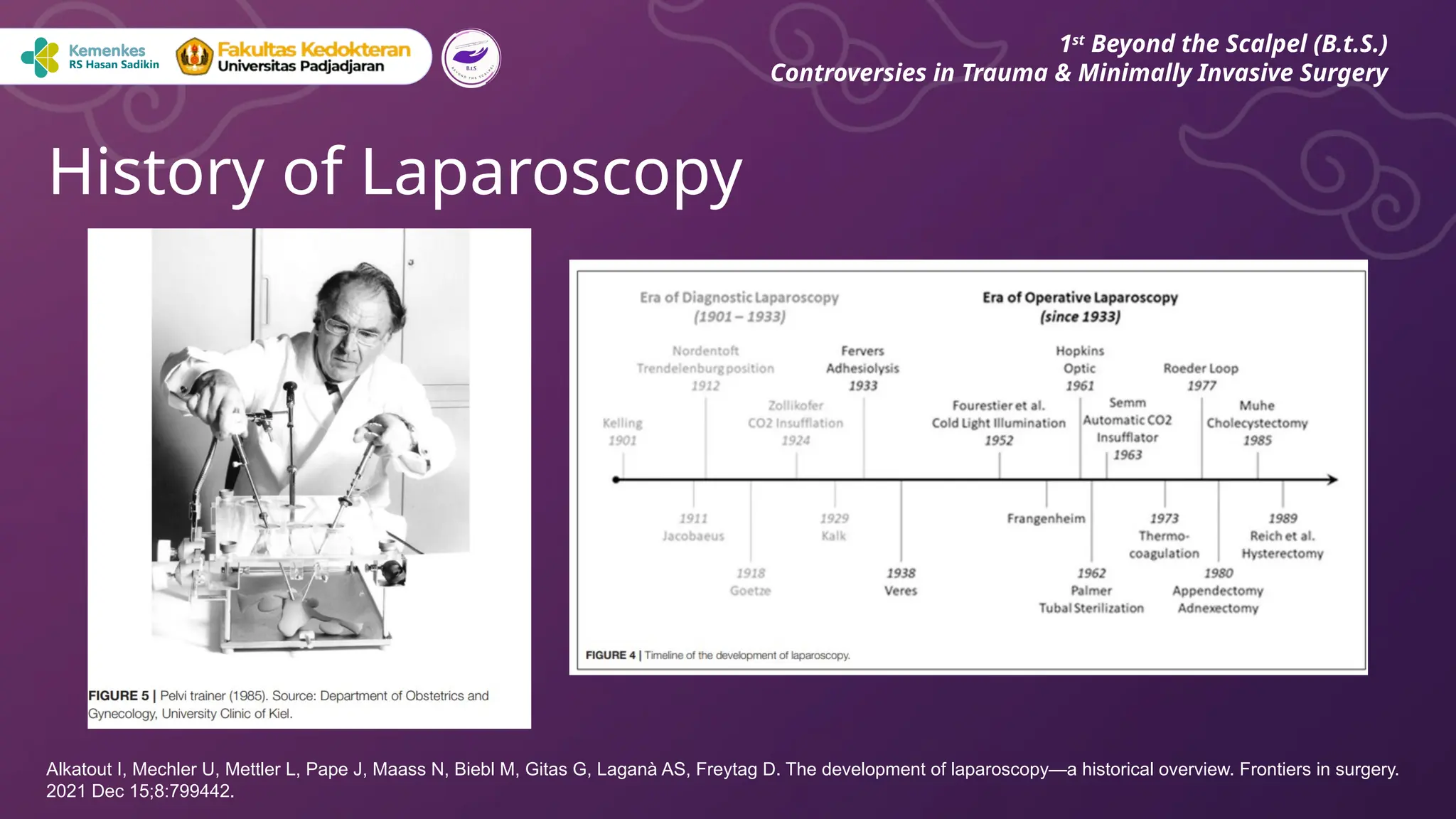
Alkatout I, Mechler U, Mettler L, Pape J, Maass N, Biebl M, Gitas G, Laganà AS, Freytag D. The development of laparoscopy—a historical overview. Frontiers in surgery.
2021 Dec 15;8:799442.
Alkatout I, Mechler U, Mettler L, Pape J, Maass N, Biebl M, Gitas G, Laganà AS, Freytag D. The development of laparoscopy—a historical overview. Frontiers in surgery.
2021 Dec 15;8:799442.
5.
History of Laparoscopy
1st
Beyondthe Scalpel (B.t.S.)
Controversies in Trauma & Minimally Invasive Surgery
Alkatout I, Mechler U, Mettler L, Pape J, Maass N, Biebl M, Gitas G, Laganà AS, Freytag D. The development of laparoscopy—a historical overview. Frontiers in surgery.
2021 Dec 15;8:799442.
6.
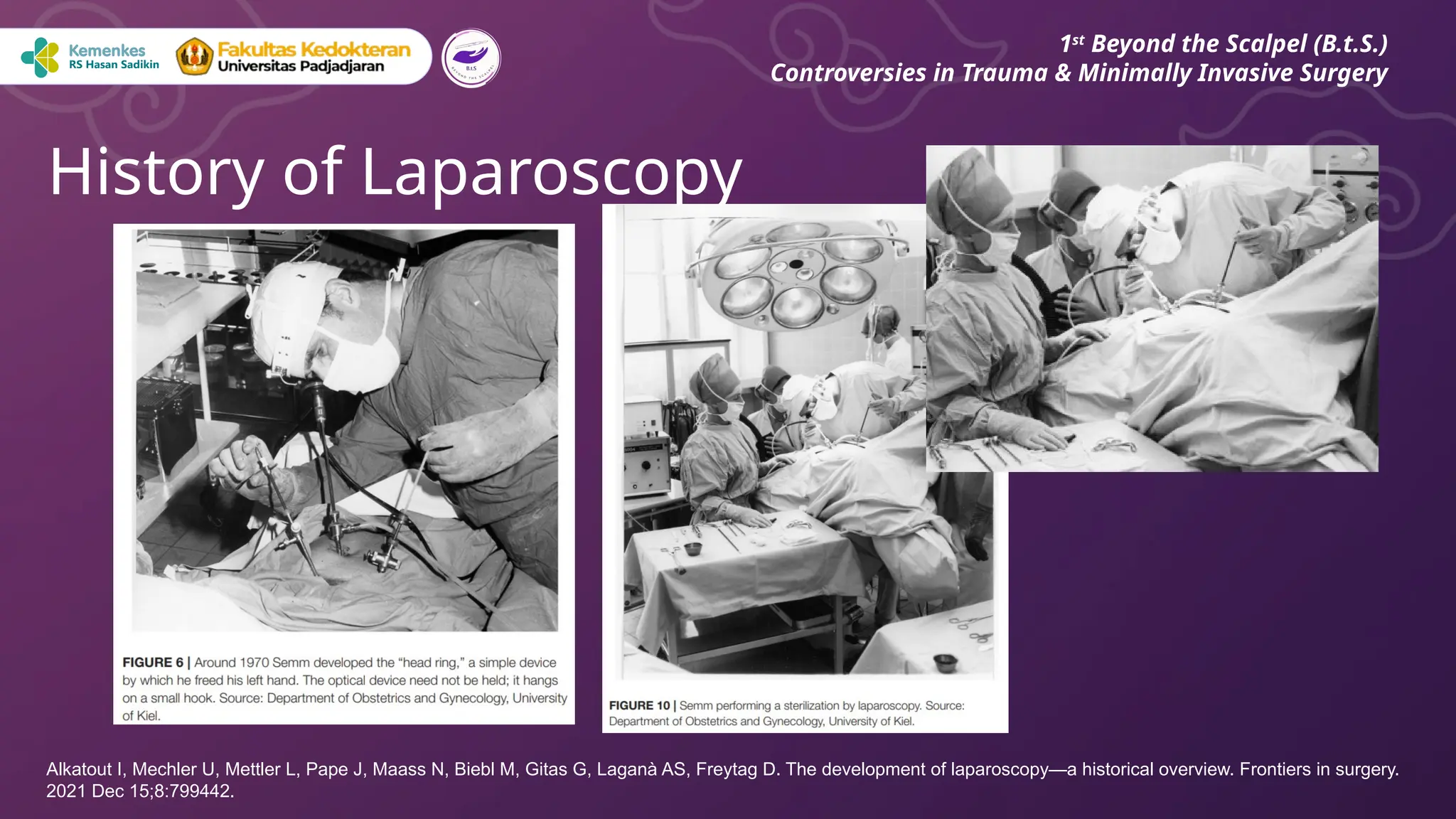
History of Laparoscopy
1st
Beyondthe Scalpel (B.t.S.)
Controversies in Trauma & Minimally Invasive Surgery
Alkatout I, Mechler U, Mettler L, Pape J, Maass N, Biebl M, Gitas G, Laganà AS, Freytag D. The development of laparoscopy—a historical overview. Frontiers in surgery.
2021 Dec 15;8:799442.
7.
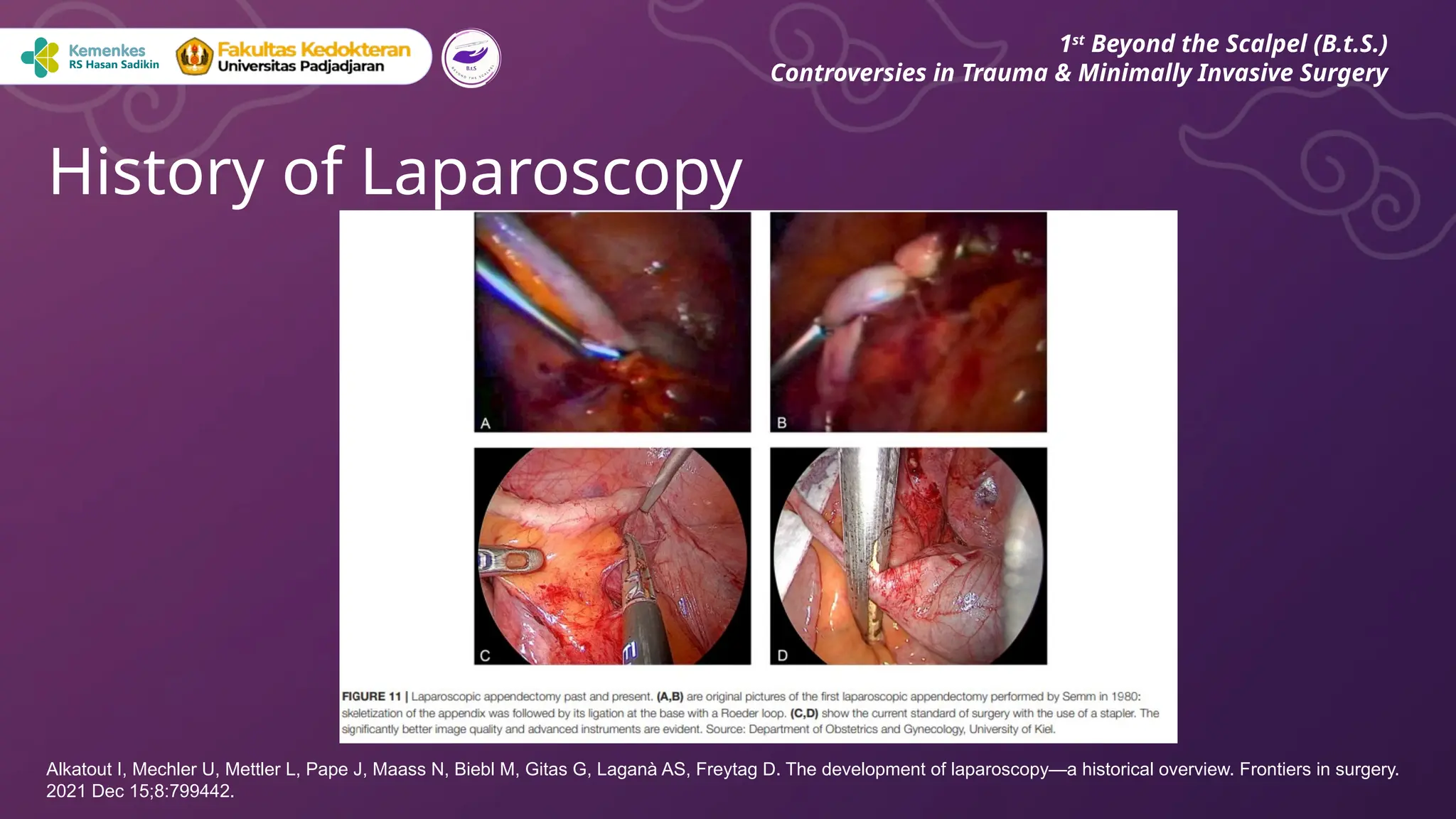
History of Laparoscopy
1st
Beyondthe Scalpel (B.t.S.)
Controversies in Trauma & Minimally Invasive Surgery
Alkatout I, Mechler U, Mettler L, Pape J, Maass N, Biebl M, Gitas G, Laganà AS, Freytag D. The development of laparoscopy—a historical overview. Frontiers in surgery.
2021 Dec 15;8:799442.
8.
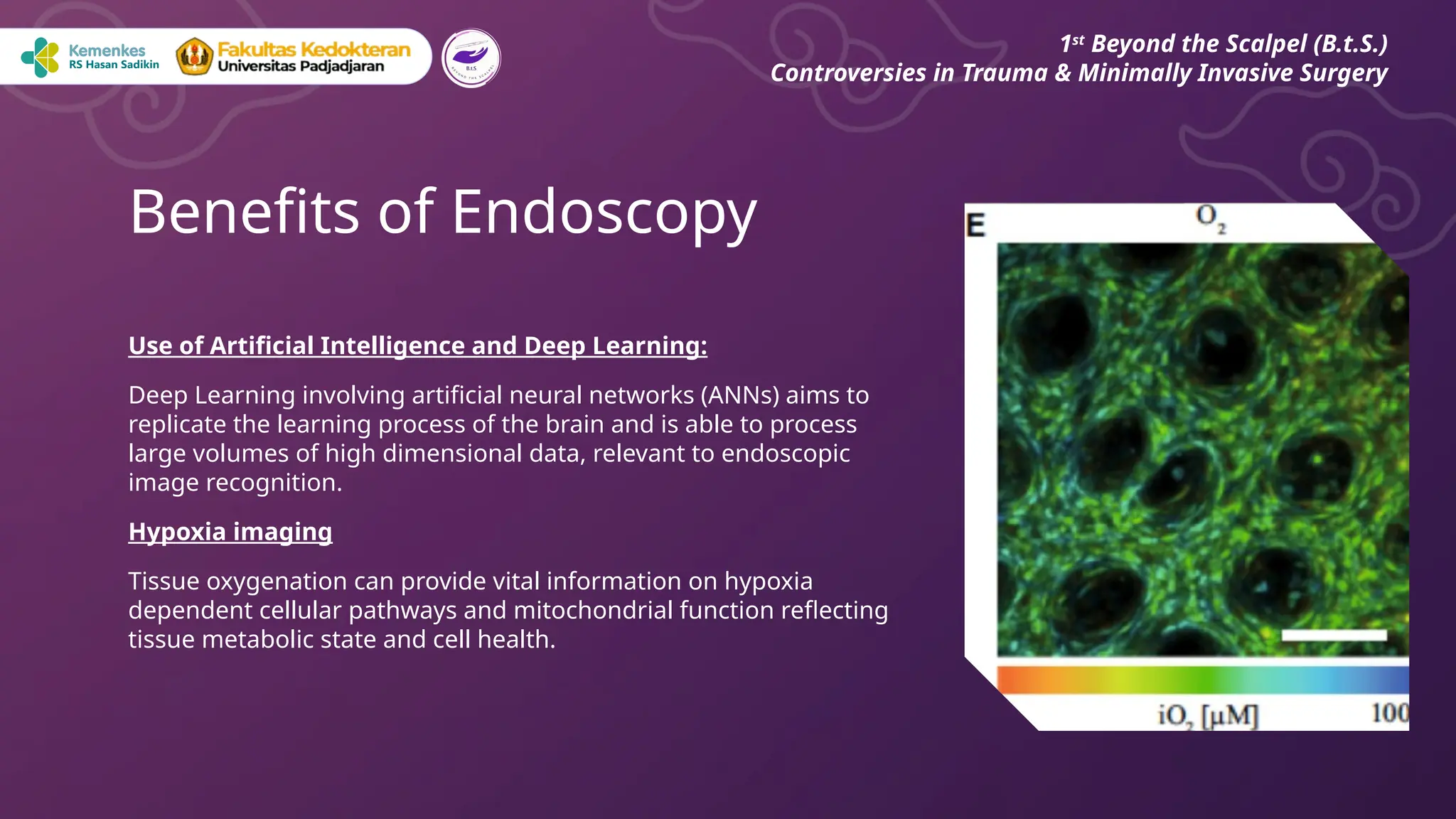
Use of ArtificialIntelligence and Deep Learning:
Deep Learning involving artificial neural networks (ANNs) aims to
replicate the learning process of the brain and is able to process
large volumes of high dimensional data, relevant to endoscopic
image recognition.
Hypoxia imaging
Tissue oxygenation can provide vital information on hypoxia
dependent cellular pathways and mitochondrial function reflecting
tissue metabolic state and cell health.
Benefits of Endoscopy
1st
Beyond the Scalpel (B.t.S.)
Controversies in Trauma & Minimally Invasive Surgery
9.
Minimally Invasive:
● Endoscopicsurgery requires only small incisions or natural orifices, leading to less tissue damage,
reduced pain, and faster recovery times.
Reduced Risk of Complications:
● The smaller incisions lower the risk of infections and other surgical complications.
Shorter Hospital Stays:
● Patients often have shorter hospital stays and quicker returns to normal activities.
Improved Visualization:
● High-definition cameras provide magnified views of the surgical field, which can improve precision
Benefits of Laparoscopy
1st
Beyond the Scalpel (B.t.S.)
Controversies in Trauma & Minimally Invasive Surgery
10.
Complex or LargeTumors:
● Some cancers or large growths may not be accessible or treatable via endoscopy, requiring open
surgery for complete removal.
Severe Inflammation or Scar Tissue:
● Conditions like severe diverticulitis or dense adhesions from previous surgeries can make endoscopic
approaches challenging.
Emergency Situations:
● While some emergencies can be managed endoscopically (e.g., bleeding ulcers), others may need
immediate open surgery due to the need for direct access and quick action.
Dangers of Endoscopy
1st
Beyond the Scalpel (B.t.S.)
Controversies in Trauma & Minimally Invasive Surgery
11.
Structural Limitations:
● Certainanatomical structures or disease processes may not be easily reached or treated through
endoscopy. For example, some spinal surgeries or complex cardiac procedures still require open
techniques.
Learning Curve:
● Not all surgeons are trained or experienced in endoscopic methods, and there can be a steep learning
curve to master these techniques.
Dangers of Endoscopy
1st
Beyond the Scalpel (B.t.S.)
Controversies in Trauma & Minimally Invasive Surgery
12.
●Appendectomy
●Cholecystectomy
●Esophageal Surgery
●Reflux Surgery
●GastricSurgery
●Colorectal Surgery
●Colon cancer
●Rectal Surgery
Laparoscopic Surgeries
1st
Beyond the Scalpel (B.t.S.)
Controversies in Trauma & Minimally Invasive Surgery
• Rectal Cancer
• Liver Surgery
• Surgery of the adrenal glands
• Pancreatic Surgery
• Surgery of the Spleen
• Laparoscopic Hernia Surgery
Buia A, Stockhausen F, Hanisch E. Laparoscopic surgery: a qualified systematic review. World journal of methodology. 2015 Dec 12;5(4):238.
13.
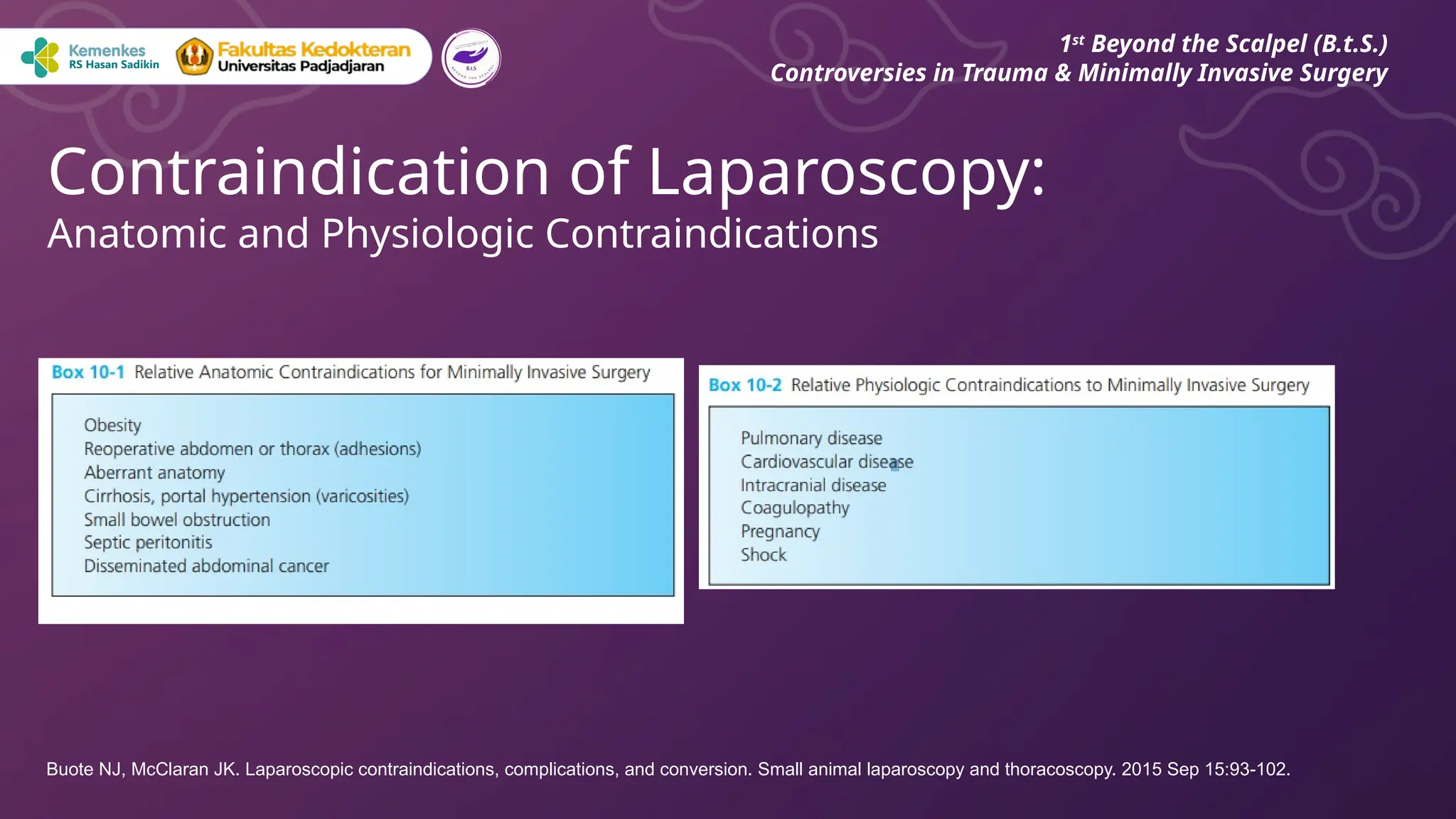
Contraindication of Laparoscopy:
Anatomicand Physiologic Contraindications
1st
Beyond the Scalpel (B.t.S.)
Controversies in Trauma & Minimally Invasive Surgery
Buote NJ, McClaran JK. Laparoscopic contraindications, complications, and conversion. Small animal laparoscopy and thoracoscopy. 2015 Sep 15:93-102.
14.
●Non-specific abdominal pain
●Acutecholecystitis
●Acute appendicitis
●Acute sigmoid diverticulitis
●Acute gallstone pancreatitis
●Acute intestinal obstruction due to pain
●Gastro-duodenal ulcer disease
Emergency Laparoscopic: Role and Implementation
1st
Beyond the Scalpel (B.t.S.)
Controversies in Trauma & Minimally Invasive Surgery
Lupinacci RM, Menegaux F, Trésallet C. Emergency laparoscopy: role and implementation. Journal of Visceral Surgery. 2015 Dec 1;152(6):S65-71.
15.
● Cost andAccessibility
○ Requires expensive specialized equipment.
○ Limits access in resource-limited areas
● Learning Curve
○ The technique has a steep learning curve.
○ Lack of experience can increase the risk of complications.
○ Requires additional time and cost for adequate training.
Controversies in Laparoscopic Surgeries
1st
Beyond the Scalpel (B.t.S.)
Controversies in Trauma & Minimally Invasive Surgery
Buia A, Stockhausen F, Hanisch E. Laparoscopic surgery: a qualified systematic review. World journal of methodology. 2015 Dec 12;5(4):238.
16.
● Hidden Risk
○Complications like internal bleeding or perforation may be hard to detect.
○ Gas insufflation can affect cardiopulmonary function
● Patient Selection
○ Not all patients are suitable for laparoscopy.
○ Patients with extensive adhesions, morbid obesity, or prior abdominal surgeries may not
benefit optimally.
Controversies in Laparoscopic Surgeries
1st
Beyond the Scalpel (B.t.S.)
Controversies in Trauma & Minimally Invasive Surgery
Buia A, Stockhausen F, Hanisch E. Laparoscopic surgery: a qualified systematic review. World journal of methodology. 2015 Dec 12;5(4):238.
17.
●Adhesion
○inability to obtainadequate exposure for the critical region of
interest
●Very large mass
○may fill the entire abdomen and limit vision and access to
organs
When to convert to laparotomy?
1st
Beyond the Scalpel (B.t.S.)
Controversies in Trauma & Minimally Invasive Surgery
Mehasseb M. Laparoscopic surgery: when to convert to laparotomy?. Gynecologic and obstetric surgery: challenges and management options. 2016 Feb 24:267-8.
18.
●Obesity
○Conversion risks arehigher with a BMI greater than 30, and
dramatically increase with a BMI greater than 50
●Hemorrhage
●Comorbid
○Pre‐existing chronic obstructive and restrictive lung diseases
When to convert to laparotomy?
1st
Beyond the Scalpel (B.t.S.)
Controversies in Trauma & Minimally Invasive Surgery
Mehasseb M. Laparoscopic surgery: when to convert to laparotomy?. Gynecologic and obstetric surgery: challenges and management options. 2016 Feb 24:267-8.
19.
Patient Preparation:
● Identifyconditions like bleeding disorders, cardiovascular issues, or allergies that may increase risks.
● Adhere to fasting guidelines to minimize the risk of aspiration.
● Use the least amount of sedation necessary for patient comfort, and monitor vital signs throughout.
Operator’s Expertise:
● Ensure the endoscopist is adequately trained in both diagnostic and therapeutic procedures.
● Familiarity with managing adverse events like perforation, bleeding, or cardiopulmonary instability is
critical.
Tips to reduce risk of complication or convertion:
1st
Beyond the Scalpel (B.t.S.)
Controversies in Trauma & Minimally Invasive Surgery
Buia A, Stockhausen F, Hanisch E. Laparoscopic surgery: a qualified systematic review. World journal of methodology. 2015 Dec 12;5(4):238.
20.
Equipment-Related Precautions
● Employstate-of-the-art endoscopes with enhanced imaging capabilities to improve precision.
● Perform routine checks and maintenance to avoid equipment-related failures during procedures.
Procedural Techniques
● Avoid excessive force or manipulation of tissues to minimize trauma.
● Continuously monitor vital signs and endoscopic views to promptly identify and address complications.
Tips to reduce risk of complication or convertion:
1st
Beyond the Scalpel (B.t.S.)
Controversies in Trauma & Minimally Invasive Surgery
Buia A, Stockhausen F, Hanisch E. Laparoscopic surgery: a qualified systematic review. World journal of methodology. 2015 Dec 12;5(4):238.
21.
Post-Procedural Care
● Monitorpatients post-procedure for signs of complications like bleeding, perforation, or infection.
● Provide comprehensive discharge instructions, including signs and symptoms of potential
complications and when to seek medical attention.
Tips to reduce risk of complication or convertion:
1st
Beyond the Scalpel (B.t.S.)
Controversies in Trauma & Minimally Invasive Surgery
Buia A, Stockhausen F, Hanisch E. Laparoscopic surgery: a qualified systematic review. World journal of methodology. 2015 Dec 12;5(4):238.
22.
Conclusion
While endoscopic techniqueshave significantly expanded the possibilities for
minimally invasive surgery, they are not a universal solution.
The choice between endoscopy, laparoscopy, open surgery, or other
methods depends on the specific condition, the patient's overall health, and
the expertise of the surgical team.
1st
Beyond the Scalpel (B.t.S.)
Controversies in Trauma & Minimally Invasive Surgery