Download to read offline


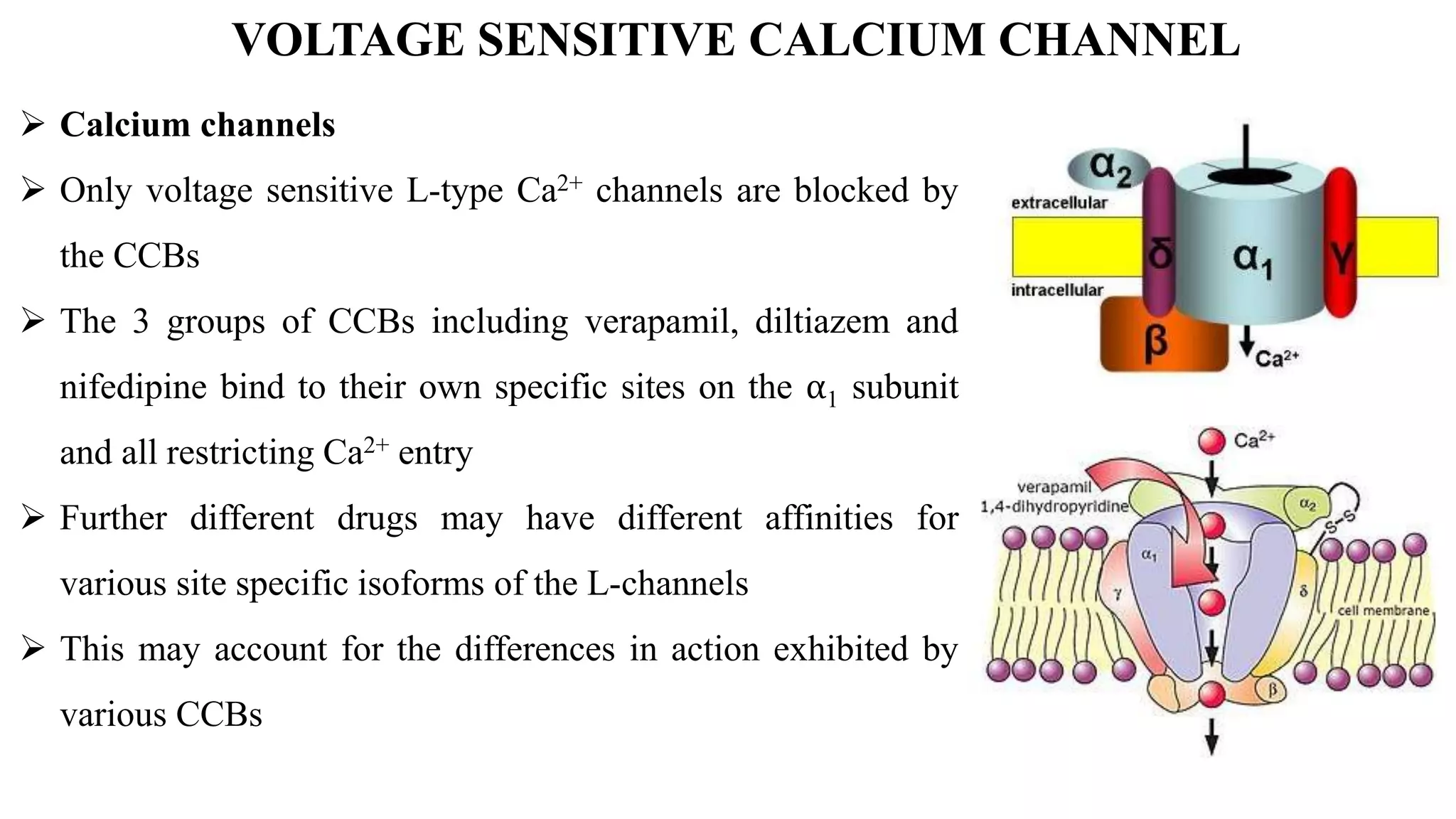
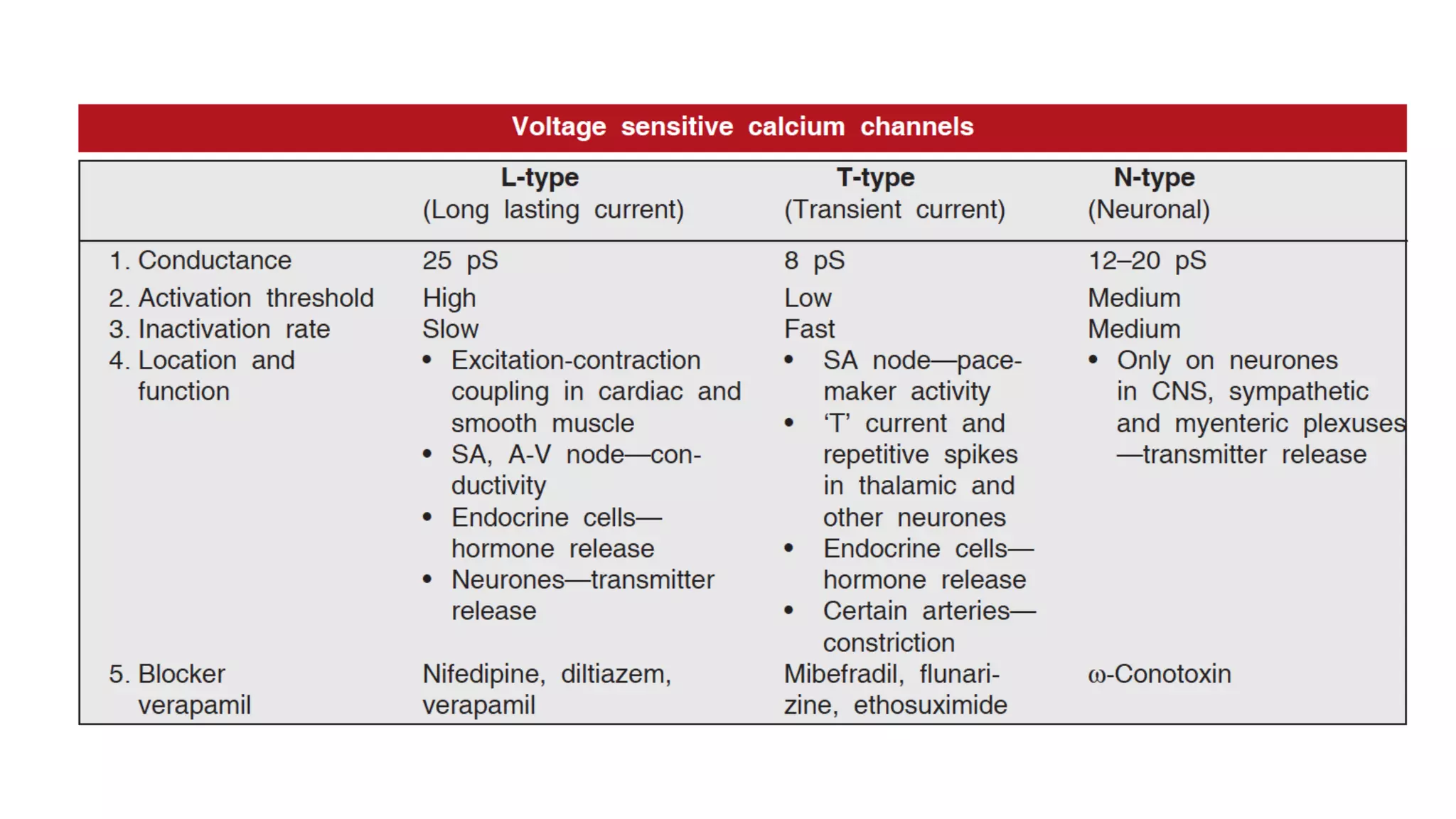
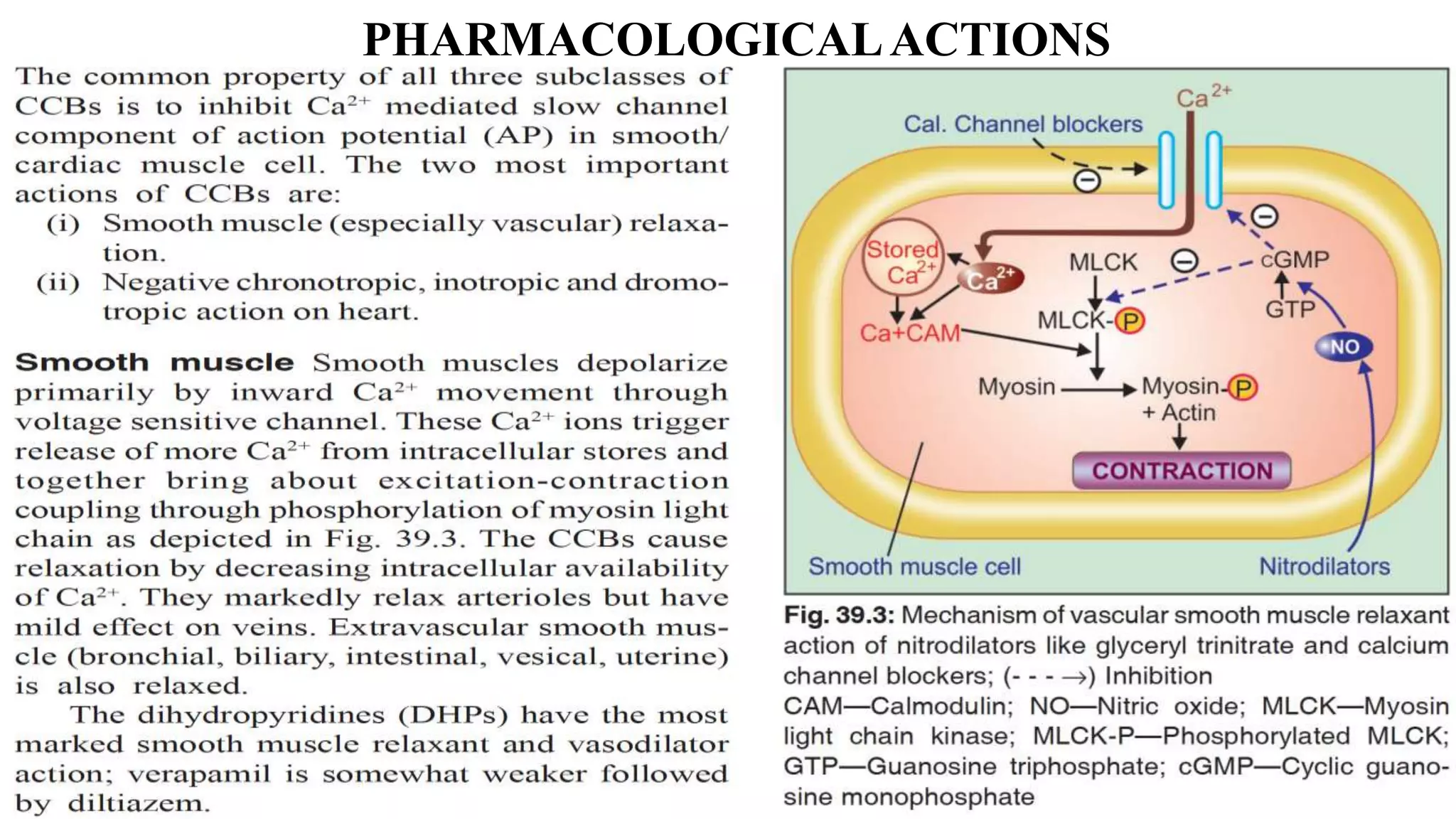
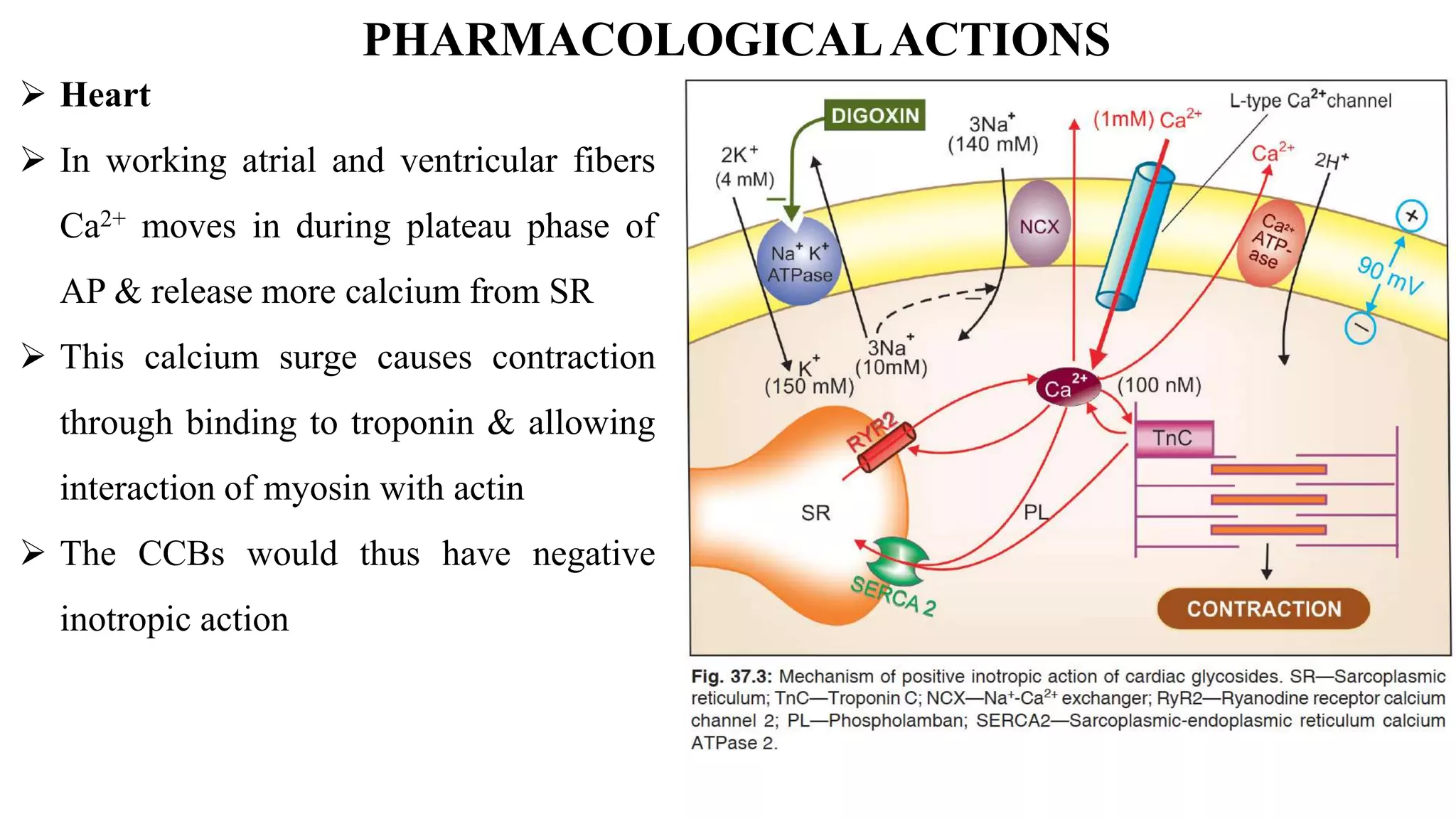
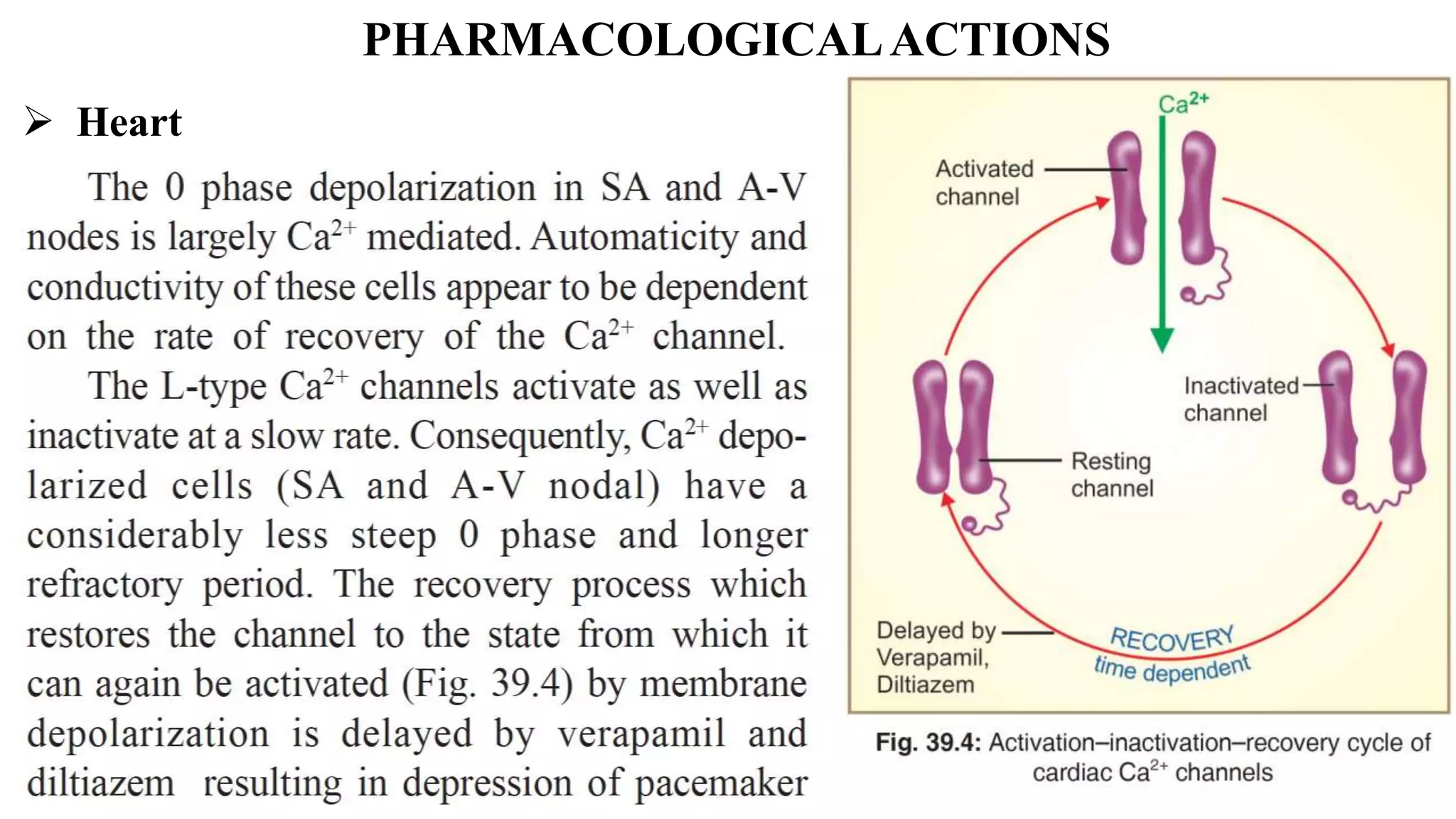



This document discusses calcium channel blockers (CCBs). It outlines three main classes of CCBs: verapamil, nifedipine, and diltiazem. Nifedipine is the most potent as a dihydropyridine. There are three types of calcium channels: voltage-sensitive, receptor-operated, and leak channels. Only the voltage-sensitive L-type calcium channels are blocked by CCBs. CCBs bind to sites on the alpha-1 subunit to restrict calcium entry, with different drugs having varying affinities for channel isoforms. CCBs have negative inotropic effects in the heart by blocking the calcium surge during the action potential plateau phase that