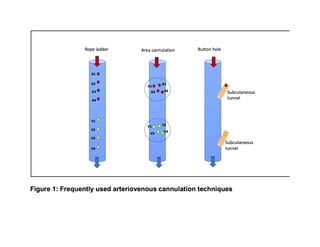
This document discusses the buttonhole cannulation technique for vascular access in hemodialysis patients. It provides a history of the technique, beginning in the 1970s in Poland. Early experiences in the US showed benefits like reduced pain, infiltration, and hematoma rates compared to rope-ladder cannulation. The technique involves creating fibrous tracts at constant needle insertion sites using repeated cannulation with sharp then blunt needles. Correct technique includes proper site selection, needle angle/depth, disinfection, and complete scab removal to prevent infection. Larger US studies are still needed to better evaluate risks and benefits.
















![1. Twardowski ZJ –Constant site (buttonhole) method of needle insertion for
hemodialysis. Dial Transplant; 24(10); 1995
2. Misra M, Toma S, Shinzato T (eds): Buttonhole Cannulation: Current Prospects
and Challenges. Contrib Nephrol. Basel, Karger, 2015, vol 186, pp 1-12
3. Twardowski Z, Lebek R, Kubara H. Six-year experi-ence with the creation and
use of internal arterio-venous fi stulae in patients treated with repeated
hemodialysis [in Polish]. Pol Arch Med Wewn. 1977;57:205-214.
4. Twardowski Z, Kubara H. Different sites versus constant sites of needle insertion
into arteriovenous fi stulas for treatment by repeated dialysis. Dial Transplant.
1979;8:978-980.
5. Kranung G. Plastic defonnation of Cimino fi stula by repeated puncture. Dial
Transplant. 1984;13:635-638.
6. Ball LK. The buttonhole technique for arteriovenous fistula cannulation. Nephrol
Nurs J. 2006;33(3):299-304
7. Ball LK, Treat L, Riffle V, Scherting D, Swift L. A multi-center perspective of the
Buttonhole Technique in the Pacific Northwest. Nephrol Nurs J. 2007;34(2):234-
241
8. How to Buttonhole a Fistula-You Tube. York Teaching Hospital NHS Foundation
Trust https://www.youtube.com/watch?v=tPZt-KJodU0 (Accessed December 24,
2019)
9. Ball LK. Buttonhole technique: Strategies to reduce infections. Nephrology
Nursing Journal 37:474-477, 2010
10.Mott H, Moore H. Kinder, gentler methods of scab removal in buttonhole access.
Nephro Nursing J 38:439-443, 2011
11.Nesrallah GE, Cuerden M, Wong JHS, Pierratos A. Staphylococcus aureus
bacteremia and buttonhole cannulation: Longterm efficacy and safety of
mupirocin prophylaxis. Clin J Am Soc Nephrol 5: 1047–1053, 2010
12.Marticorena, R.M., Hunter, J., Cook, R., Kashani, M., Delacruz, J., Petershofer,
E., Goldestein, M.B. A simple method to create buttonhole cannulation tracks in a
busy hemodialysis unit. Hemodialysis International, 13: 316-321, 2009
13.Toma S et al. A time saving method to create a fixed puncture route for the
buttonhole technique. Nephro Dial Transplant 18:2118-2121, 2003
14.Marticorena RM. A simple method to create buttonhole cannulation tracks in a
busy hemodialysis unit. Hemodial Int 14: 94-95, 2009
15.Donnelly SM, Marticorena RM, Hunter J, Goldstein MB. Supercath Safety
Clampcath buttonhole creation: complication of catheter breakage Hemodial Int.
17:450-454, 2013
16.MacRae J, Tai D, Daniw M, Lee J. Letter to the editor A simple method to create
buttonhole cannulation tracks in a busy hemodialysis unit. Hemodial Int 14:94-95,
2010
17.Birchenough, E., et al. (2010). "Buttonhole cannulation in adult patients on
hemodialysis: an increased risk of infection?" Nephrol Nurs J 37(5): 491-498, 555
18.Chan, M. R., et al. (2014). "The effect of buttonhole cannulation vs. rope-ladder
technique on hemodialysis access patency." Semin Dial 27(2): 210-216
19.Moore, T., et al. (2019). "Arteriovenous Buttonhole Access Cannulation in
Pediatric Patients on Hemodialysis." Nephrol Nurs J 46(4): 407-411](https://image.slidesharecdn.com/butenhole-201020101502/85/Butenhole-18-320.jpg)

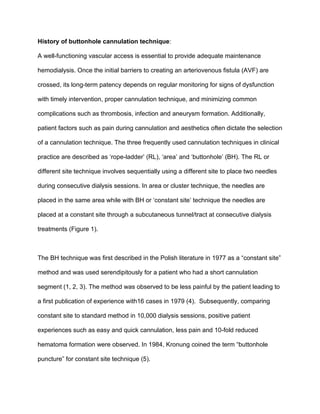
![Category Response from focus group participant
Patient
Selection
“It needs to be the right patient at the right time.”
“Home patients are more attentive.”
“Currently patients who dialyze at home are in the top tier of self-
motivation and are currently self-selected. As we increase home
dialysis, it will be essential to adapt current practices to allow for
more patients who [may not fit these criteria].”
Modality
Specific
“Fewer patients would be able to choose home if they can’t use
buttonholes.”
“Buttonholes should not be created for in-center patients, there is
a lot of infection historically, but it’s okay for home patients.”
Technique and
Training
“There should be a checklist for buttonhole cannulation.”
“Multiple cannulators increase the risk of infection, for example,
when there is an in-center creation by clinic staff before the patient
is sent home.”
“Strict aseptic technique needs to be followed (do not use “scab
removers”).”
Best Practices
Guidance
“NTDS should create a buttonhole registry.”
“If NTDS would come up with a position or recommendations on
using buttonholes, [we] would go with that.”
Table 1: Nephrologists Transforming Dialysis Safety Focus Group responses
from nephrologists and advanced practice providers](https://image.slidesharecdn.com/butenhole-201020101502/85/Butenhole-20-320.jpg)