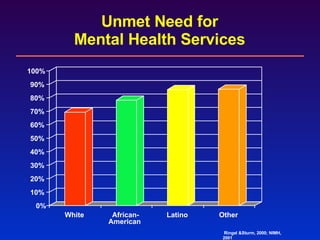
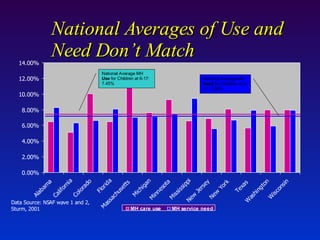
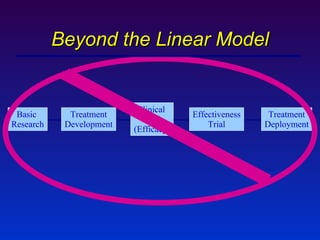
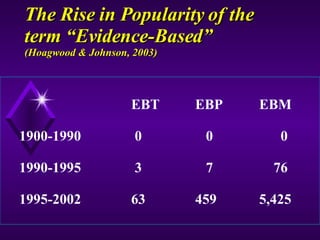
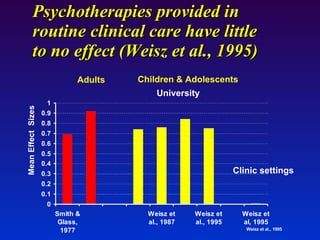
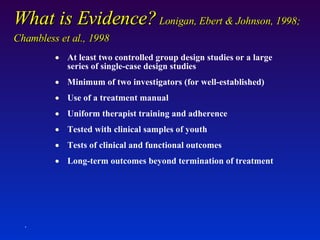
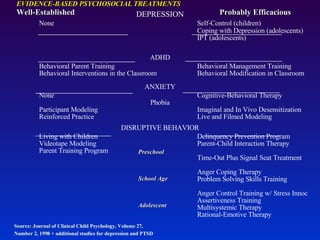
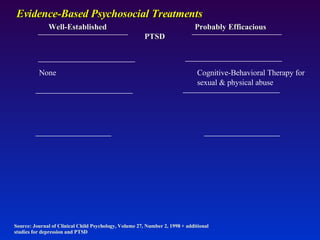
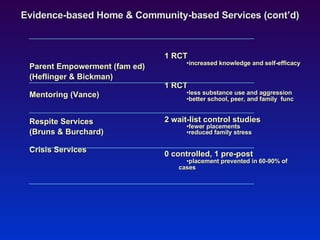
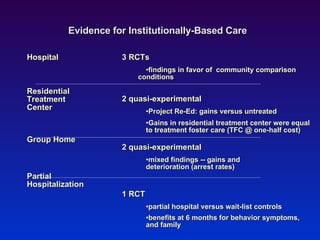
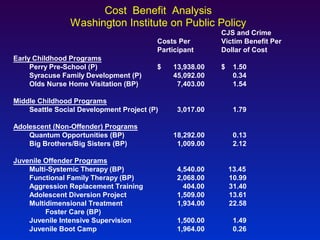
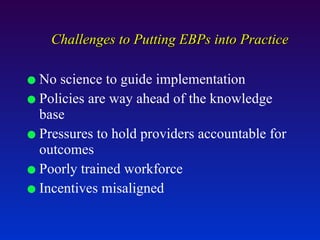
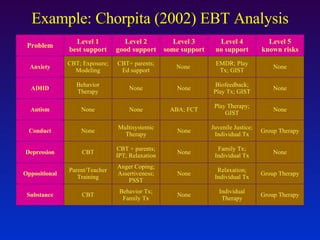
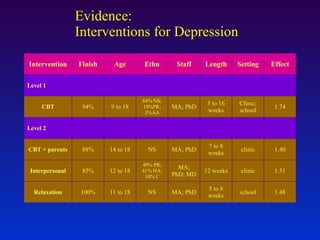
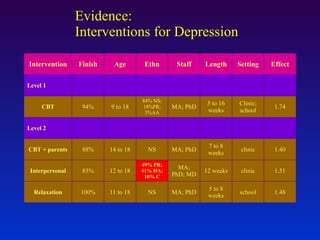
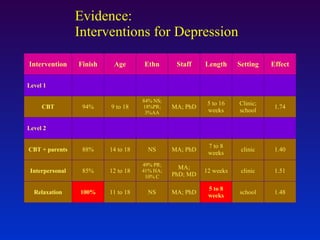
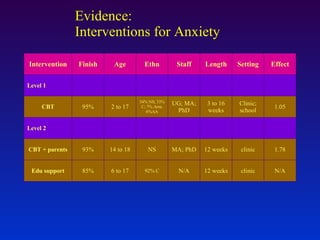
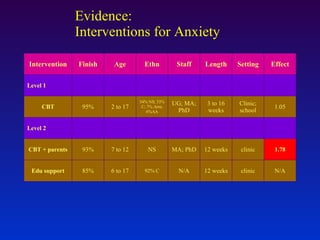
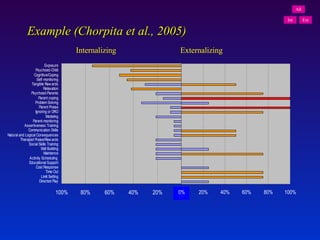
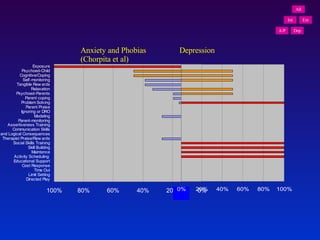
The document discusses the history and current state of evidence-based practices in children's mental health. It notes that while research has identified hundreds of evidence-based therapies and interventions, many children still have unmet mental health needs. It summarizes the levels of evidence for different psychosocial and pharmacological treatments, as well as home- and community-based services. However, it states that significant challenges remain in implementing evidence-based practices into real-world mental health systems and services.


















































![Nick Axford - evidence-based prevention [March 7 ADEPIS seminar]](https://cdn.slidesharecdn.com/ss_thumbnails/namentorukliverpool7thmarch2016-160316151401-thumbnail.jpg?width=640&height=640&fit=bounds)





























![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


















