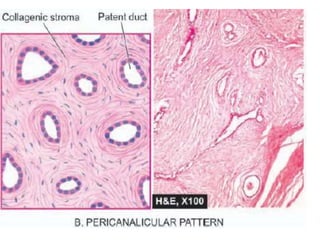
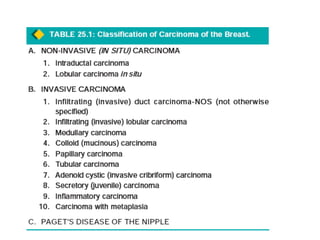
This document discusses various types of breast tumours, including benign and malignant tumours. It describes fibroadenoma as the most common benign breast tumour, occurring typically in young women aged 15-30 years. It also discusses carcinoma of the breast, which it notes is one of the most common cancers worldwide. The document outlines the risk factors for breast cancer including genetic factors, excess estrogen exposure, family history, and lifestyle factors. It then describes the different types of breast cancer in more detail, distinguishing between in situ (non-invasive) and invasive forms, with infiltrating ductal carcinoma being the most common type of invasive breast cancer.





















































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)















