This document summarizes a presentation on genetic testing for cancer risk. The presentation covered:
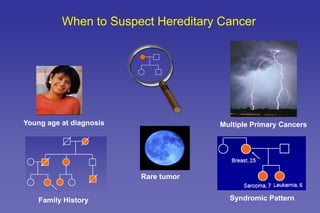
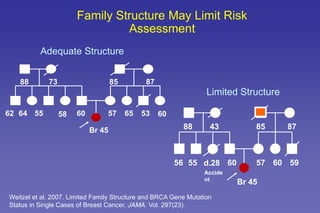
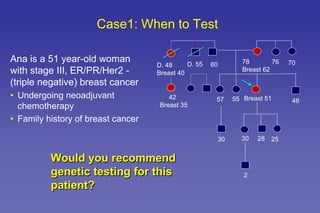
- The role of genetic cancer risk assessment in identifying inherited cancer risk.
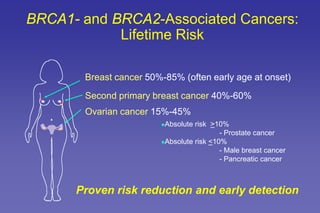
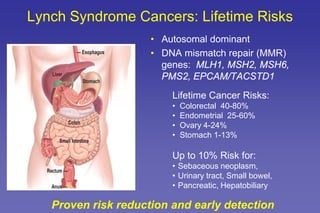
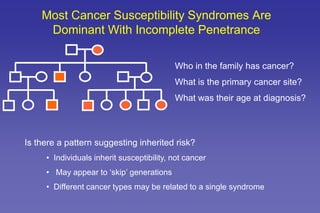
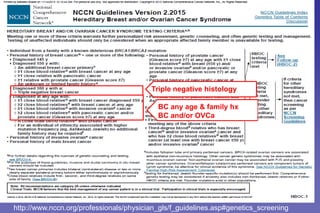
- Common hereditary cancer syndromes like BRCA1/2 and Lynch syndrome and their associated cancer risks.
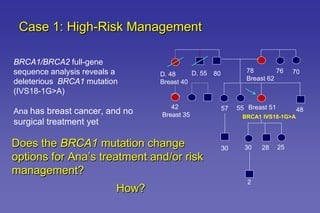
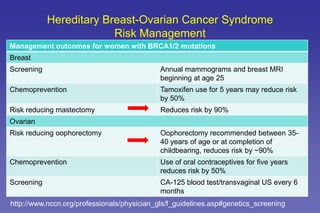
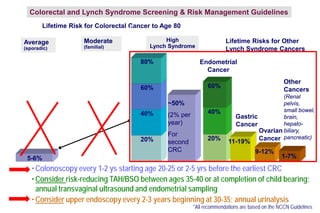
- Guidelines for cancer screening and management based on genetic test results.
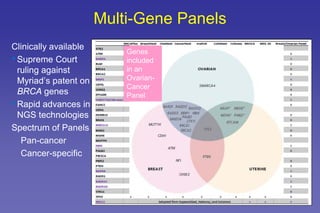
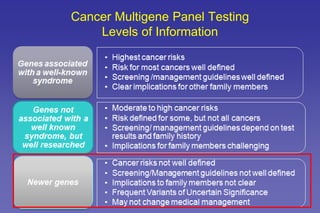
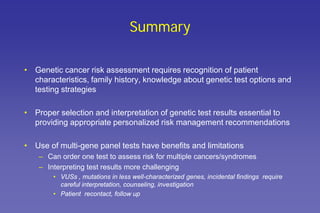
- The benefits and limitations of multi-gene cancer panels.
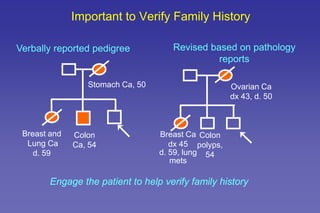
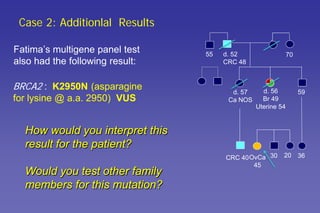
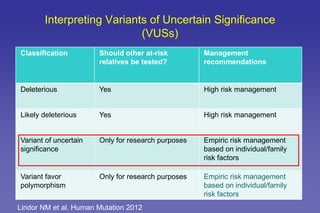
- How to interpret genetic test results and provide appropriate risk management recommendations to patients.




![HEREDITARY BREAST and OVARY CANCER [HBOC] SYNDROME, Dr BUI DAC CHI.](https://cdn.slidesharecdn.com/ss_thumbnails/hboc1-150312034459-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)






















































































