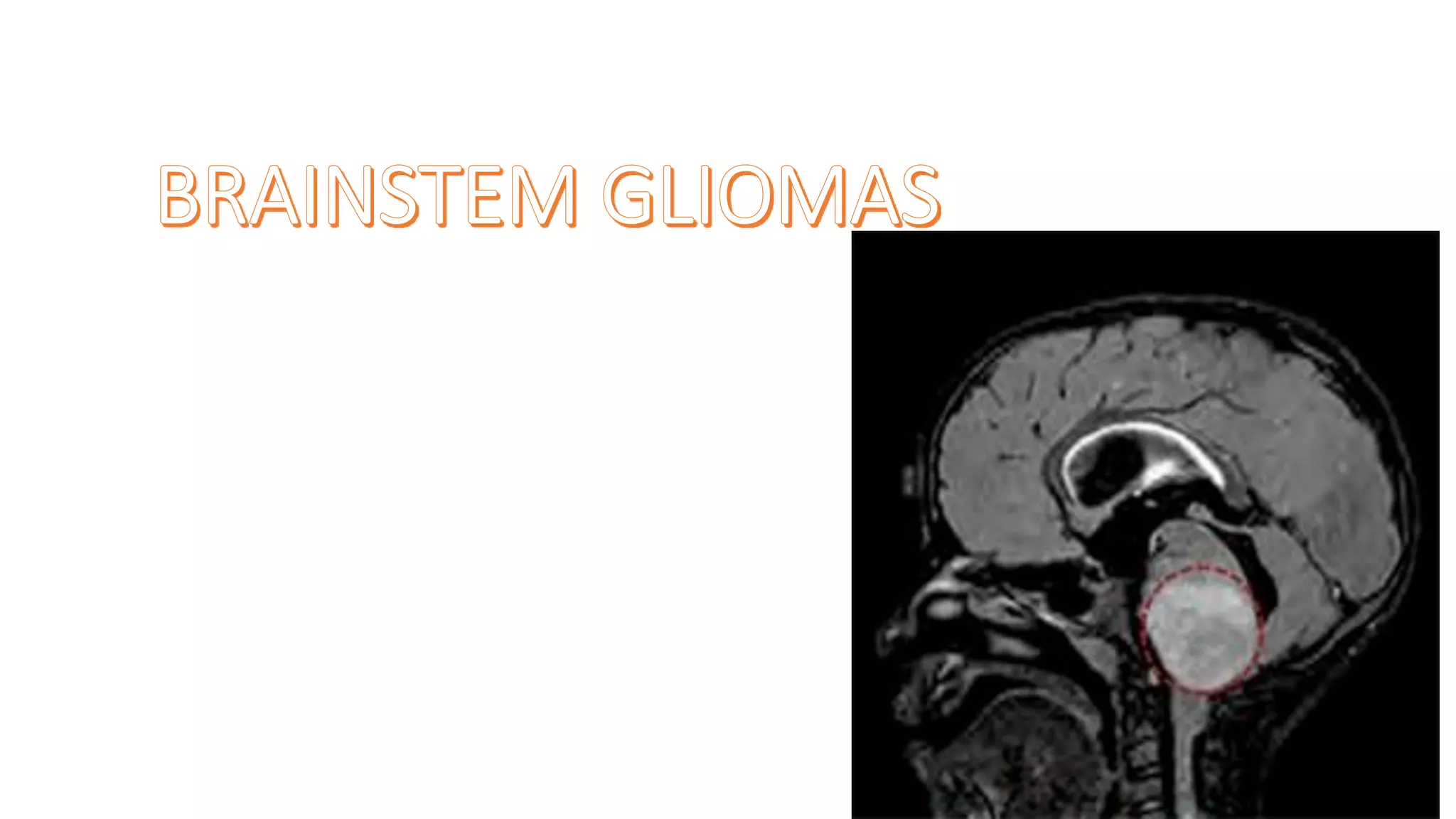
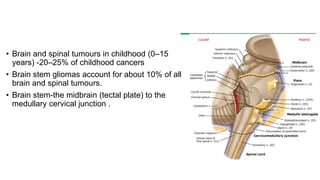
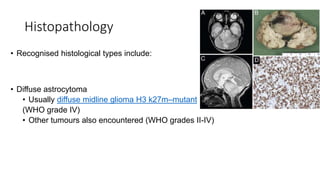
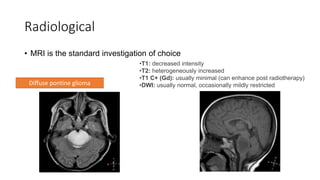
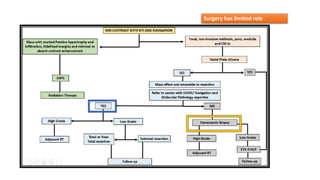
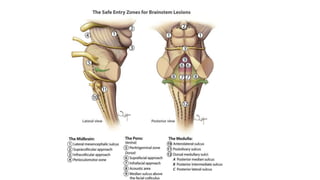
Brainstem gliomas account for about 10% of childhood brain and spinal tumors. They are challenging to treat due to their critical location. Radiation therapy plays a key role in management as surgery has limited effectiveness. Diffuse pontine gliomas, the most common type, have a terrible prognosis with over 90% of children dying within 2 years despite treatment. New immunotherapies and targeted therapies are being investigated as potential treatments to improve outcomes for these difficult to treat tumors.































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)











