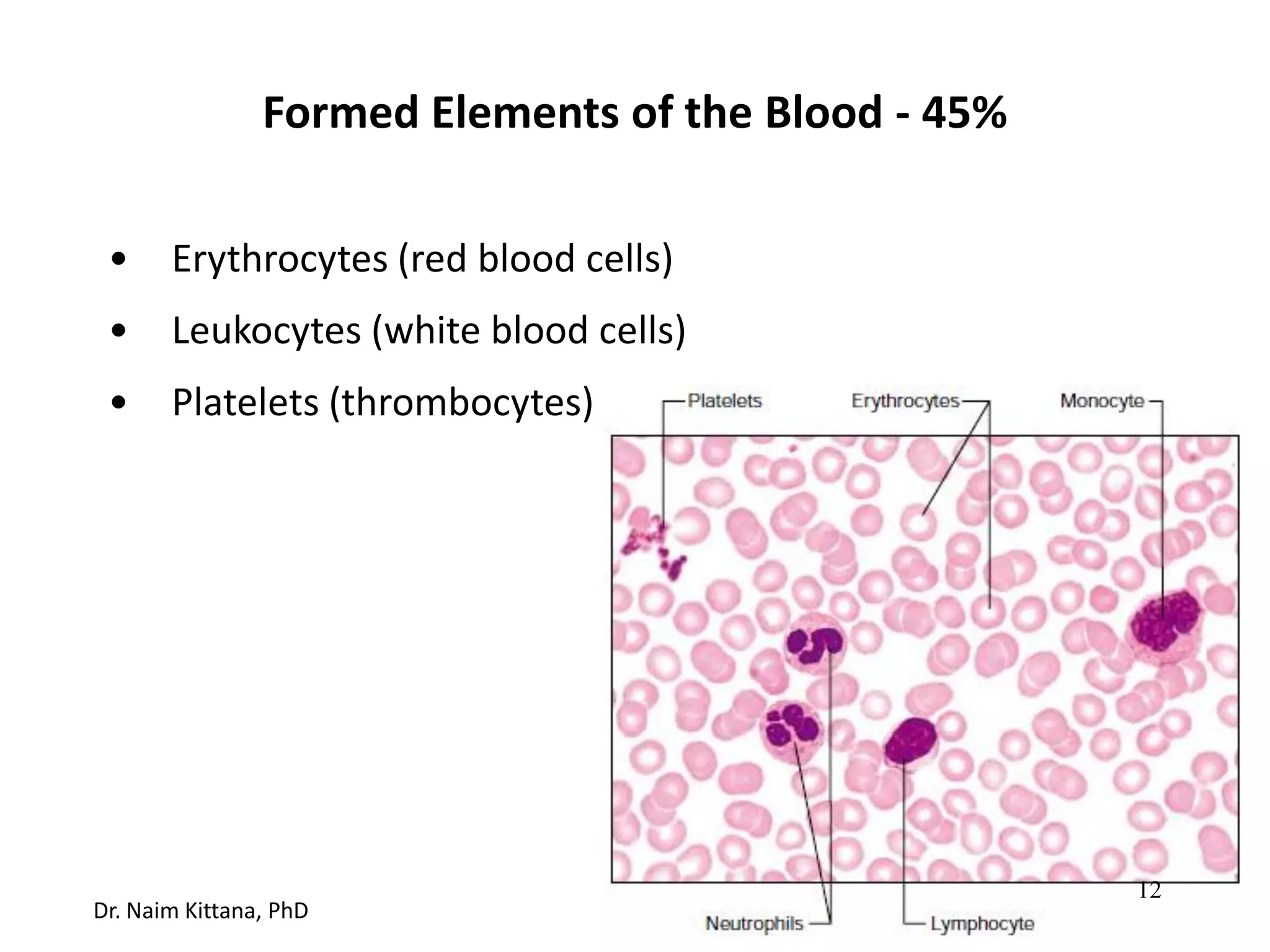
This document summarizes the physiology and anatomy of blood. It describes the components of blood including plasma, red blood cells, white blood cells, and platelets. It discusses the functions of blood in delivering oxygen, removing waste, temperature regulation, protection from blood loss and infection, and transporting hormones. The document outlines erythrocyte formation through erythropoiesis and the regulation of red blood cell production by erythropoietin. It also covers common blood disorders like anemia, hemolytic disorders like sickle cell anemia, and polycythemia.