Downloaded 83 times

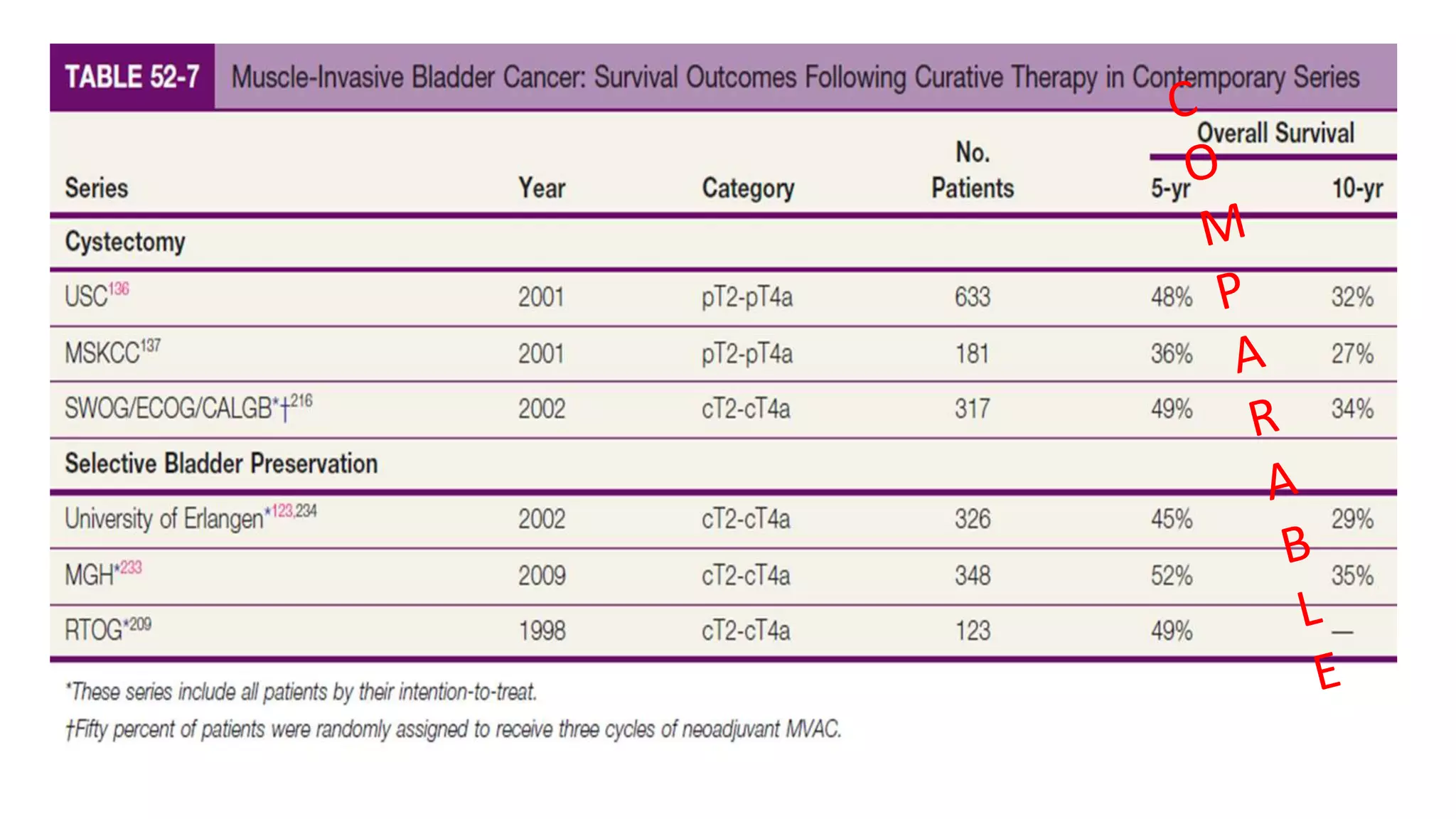
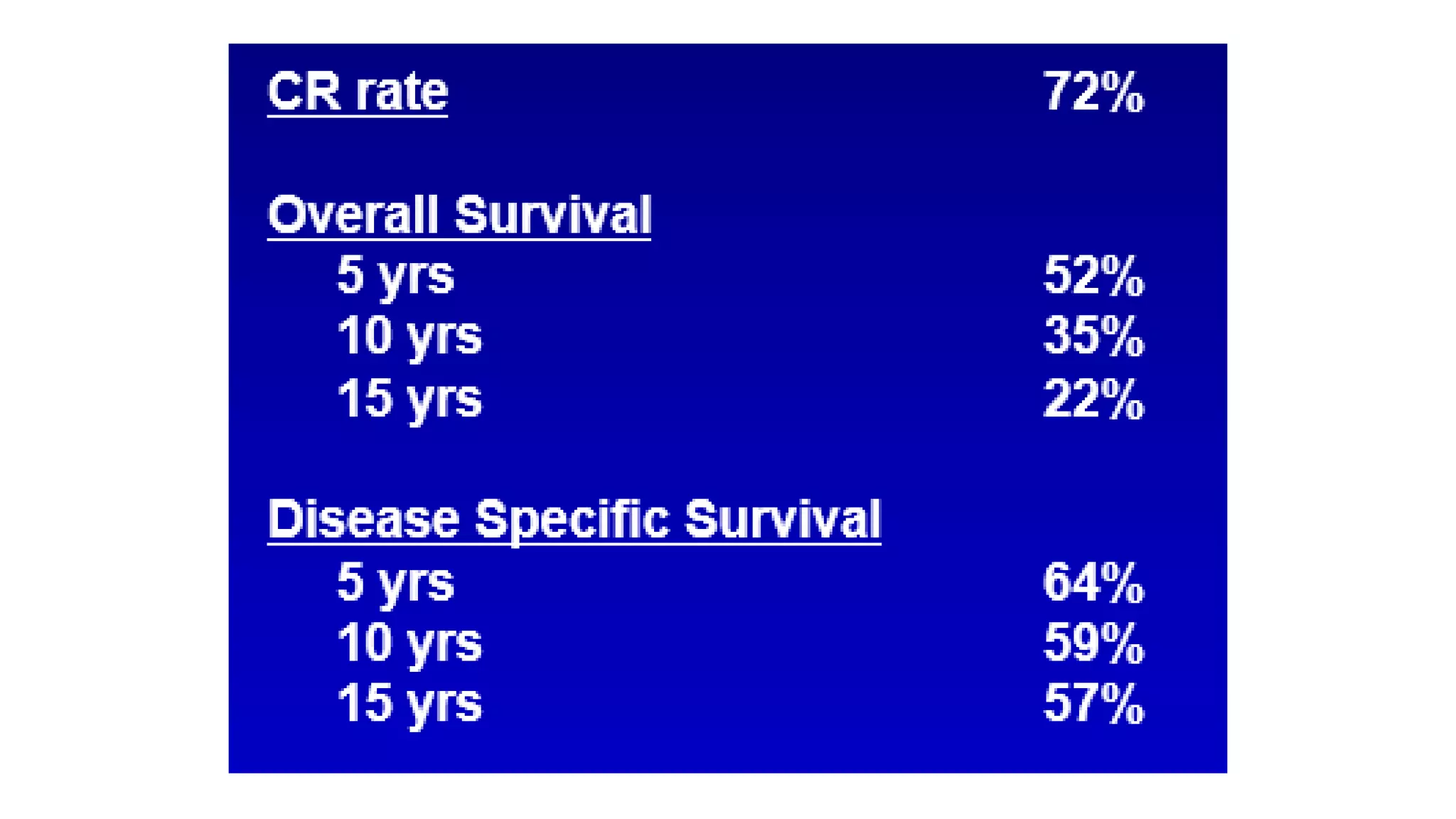
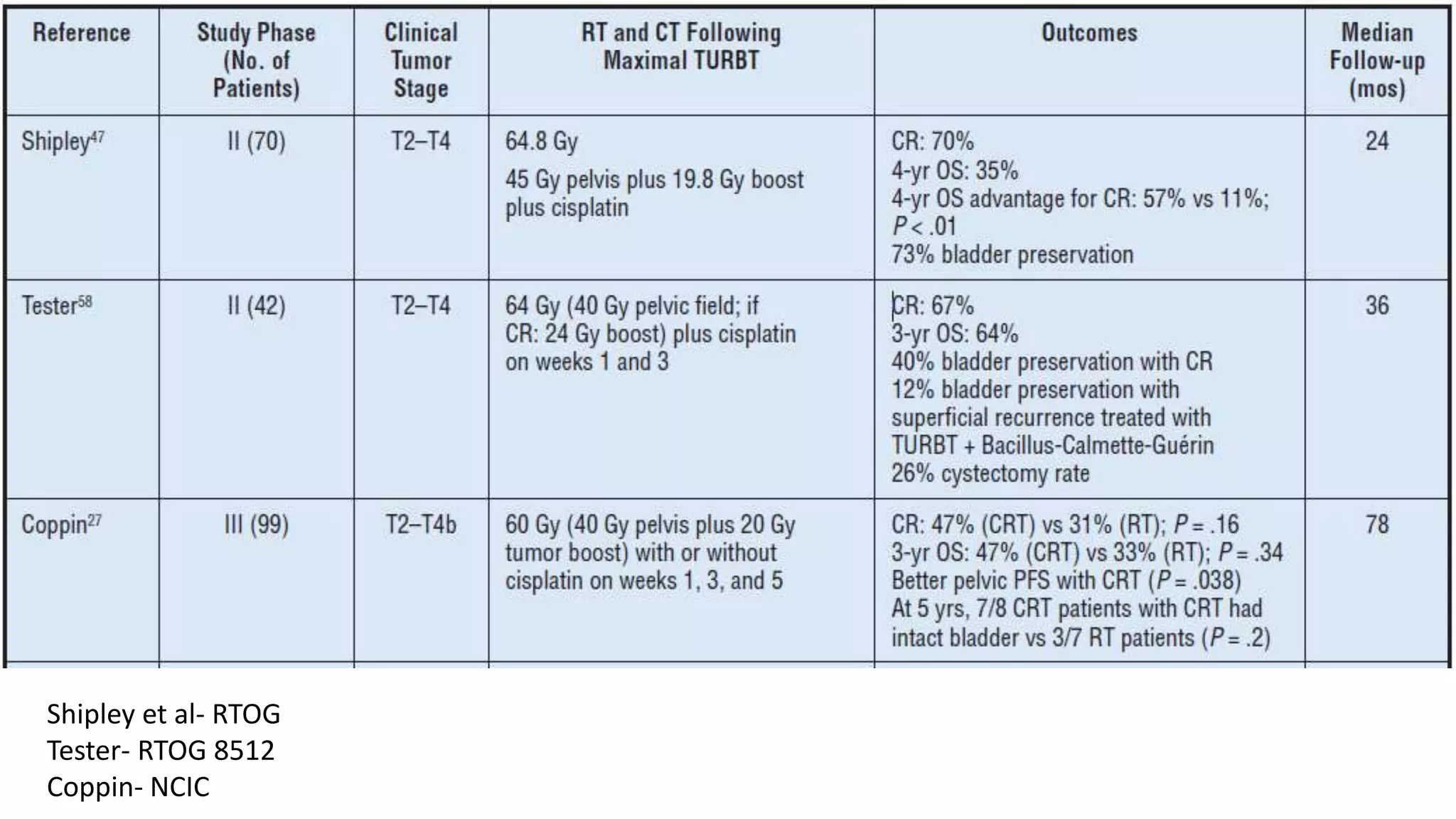
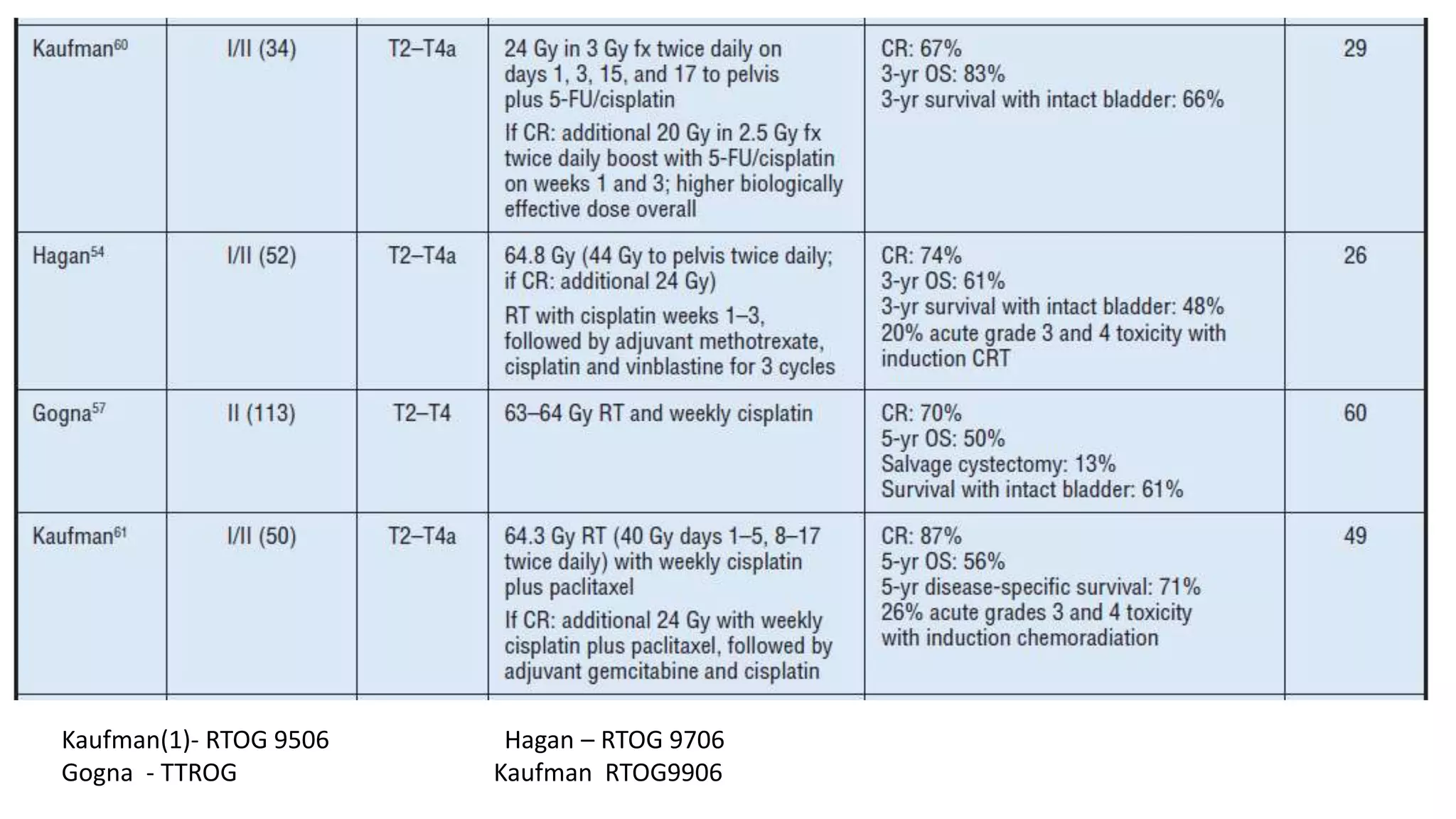
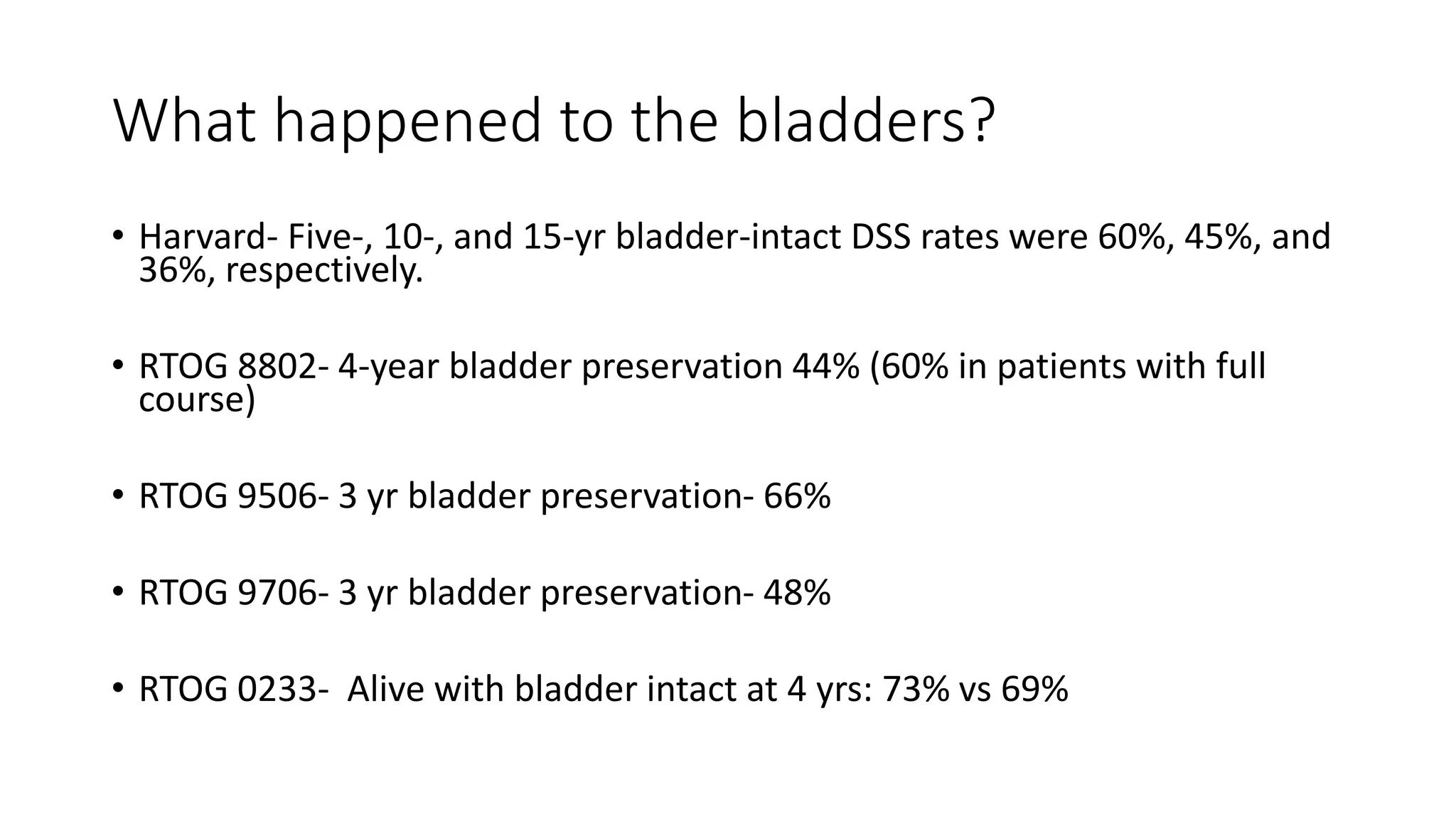

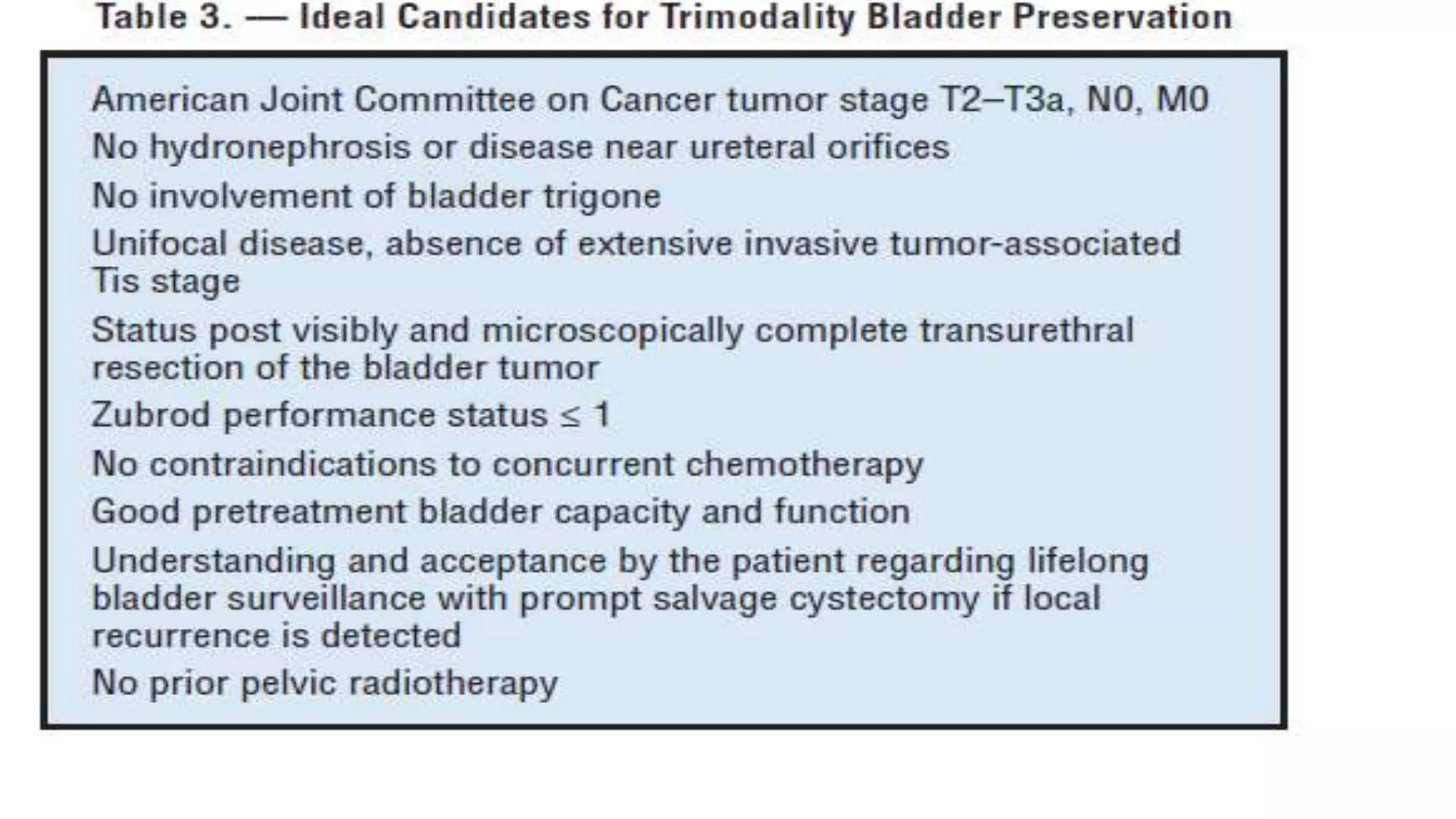
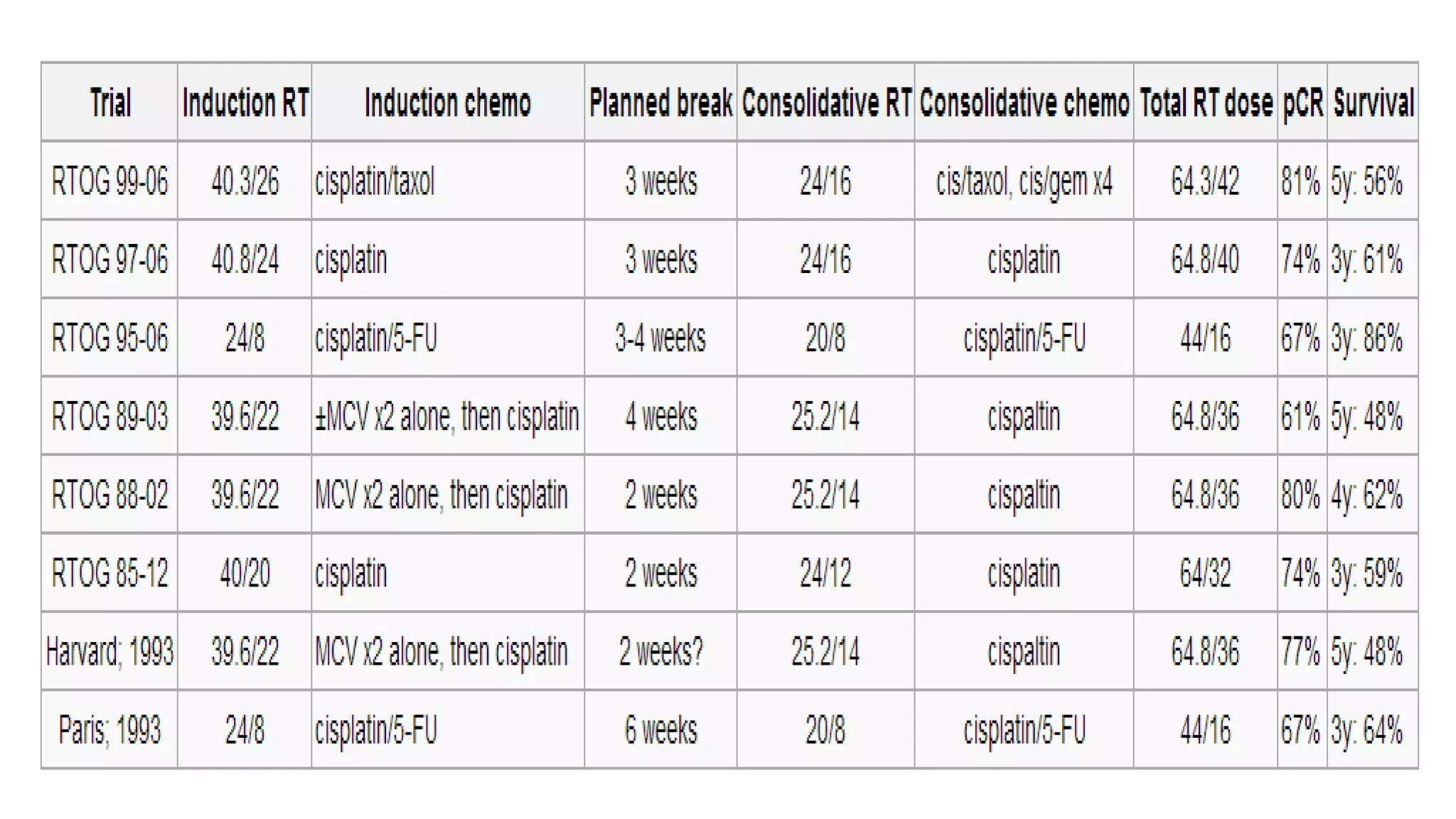

This document discusses bladder preservation as an alternative to radical cystectomy for muscle-invasive bladder cancer (MIBC). It outlines the trimodality approach of maximal transurethral resection of bladder tumor (TURBT) followed by concurrent chemoradiation. Studies have shown 5-year bladder intact survival rates ranging from 36-66% with this approach. Complete response to induction chemoradiation may allow bladder preservation. Radical cystectomy is associated with significant morbidity while bladder preservation maintains quality of life. Long-term outcomes depend on patient selection and a multidisciplinary approach can maximize organ preservation while achieving high cure rates.
































![Muscle invasive bladder Cancer [Dr.Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/muscleinvasivebladdertumoredmond-140716213247-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)


































