Downloaded 10 times



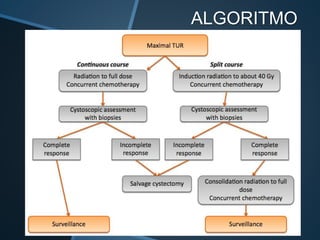


This document discusses treatment options for muscle-invasive bladder cancer, including radical cystectomy, partial cystectomy, radiotherapy alone, chemotherapy, and trimodal therapy (transurethral resection, chemotherapy, and radiotherapy). It reviews the results of four phase III trials comparing radiotherapy with and without chemotherapy. It also discusses organ preservation rates, oncological outcomes, and quality of life outcomes associated with different treatments. The document concludes that trimodal therapy with transurethral resection followed by chemoradiation based on cisplatin is an option for select patients with T2 bladder cancer without other risk factors, as it can achieve cancer-specific survival rates of 50-82% at 5 years while preserving




















































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)















