Download to read offline
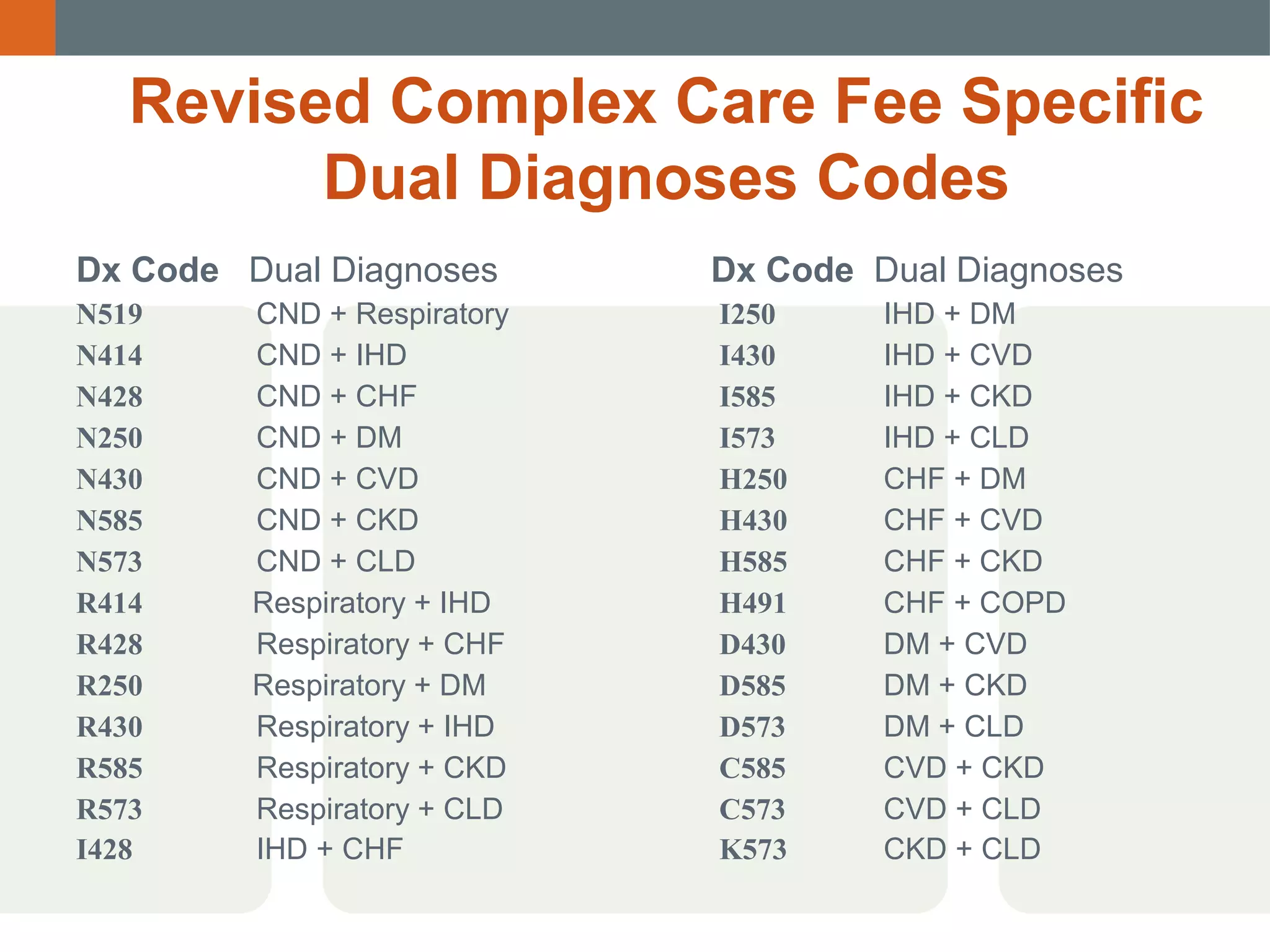
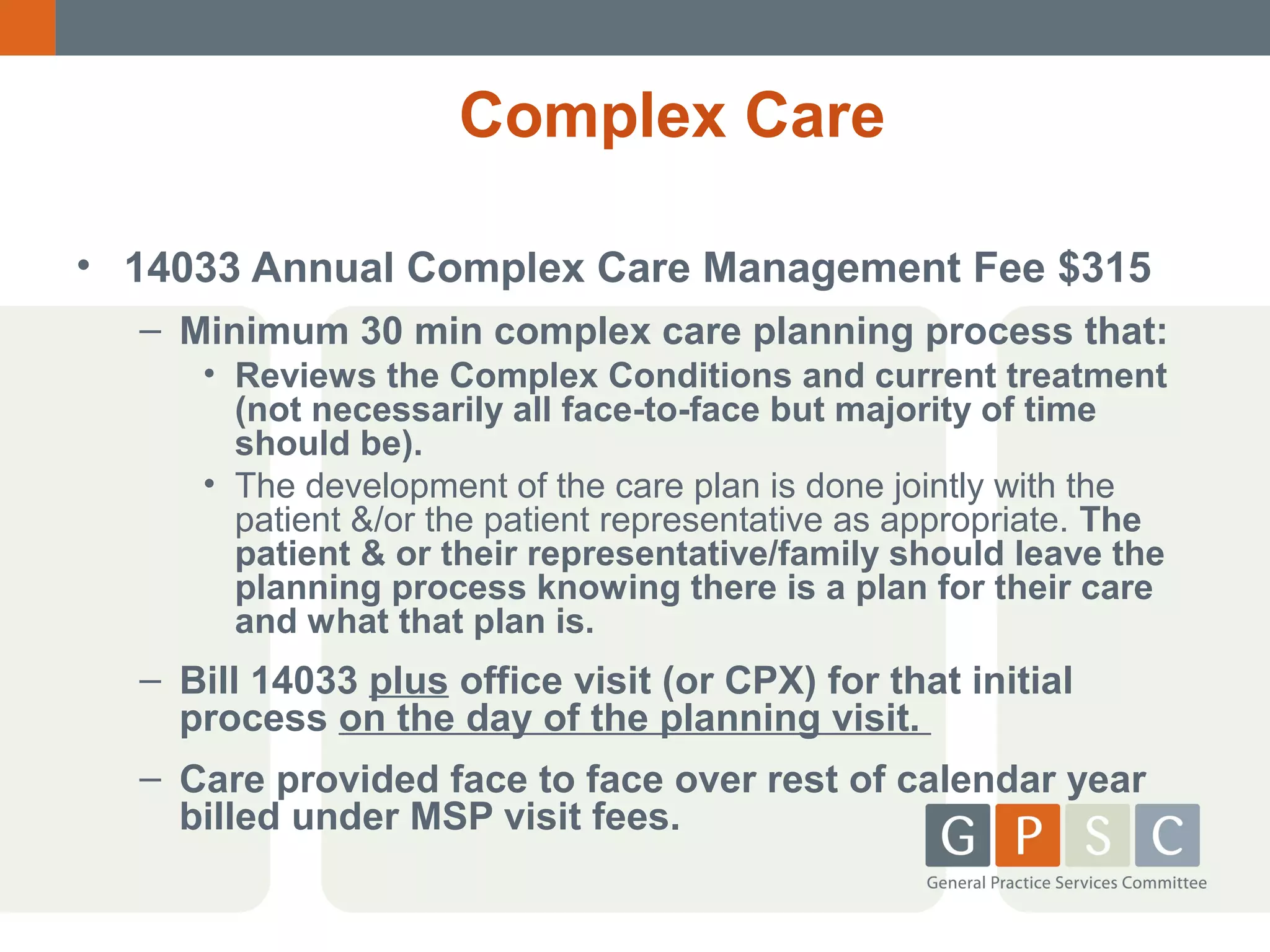
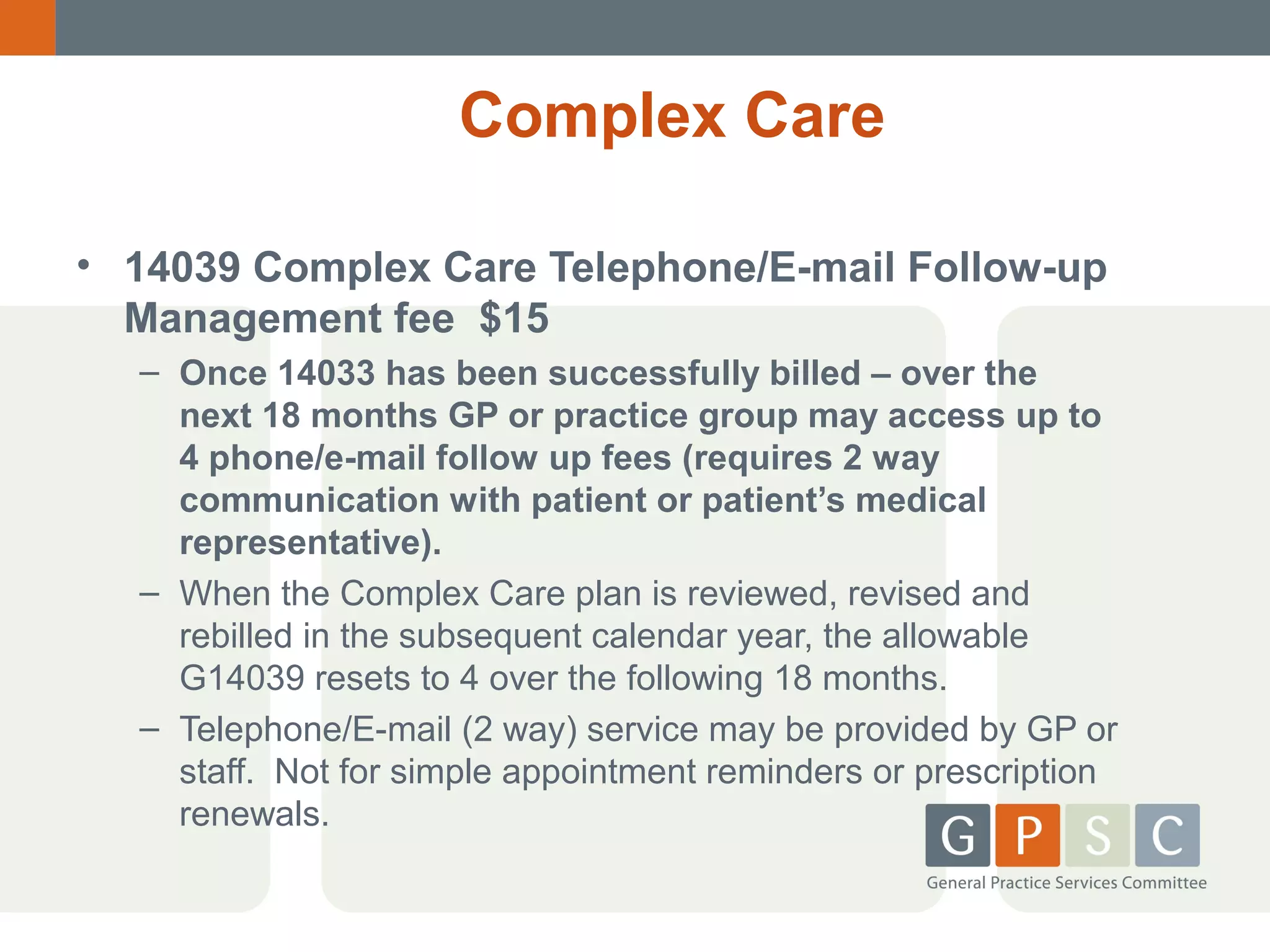

This document provides an overview and updates on GPSC and related MSP fees in British Columbia. It discusses fees for chronic disease management, complex care, conferencing, palliative care, mental health initiatives, and prevention. Key points covered include eligibility requirements for each fee code, allowable billing practices, and changes to fee codes over time. Resources for staying up-to-date on fee schedules and guidelines are also listed.










































































































