





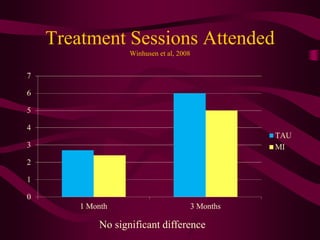
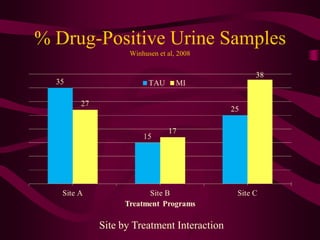
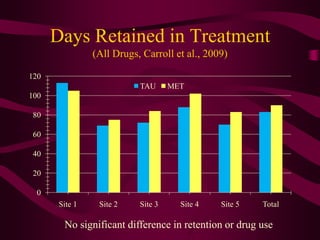
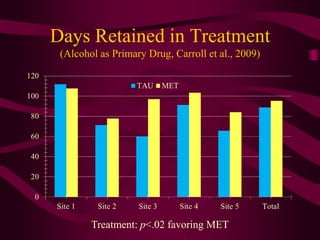
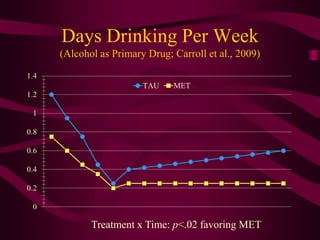

MET vs TAU in 4 large multisite RCTs found: 1) No main effect on retention or substance use for outpatient treatment. 2) One study found a small effect on early retention but not substance use. 3) Studies of pregnant drug users and Spanish speakers also found no main effects of MET vs TAU. The findings suggest MET may not produce meaningful improvements over TAU in typical substance abuse treatment settings based on these high quality trials.







































![Measures and feedback 2013 [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/measuresandfeedback2013compatibilitymode-130123185123-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)






















































