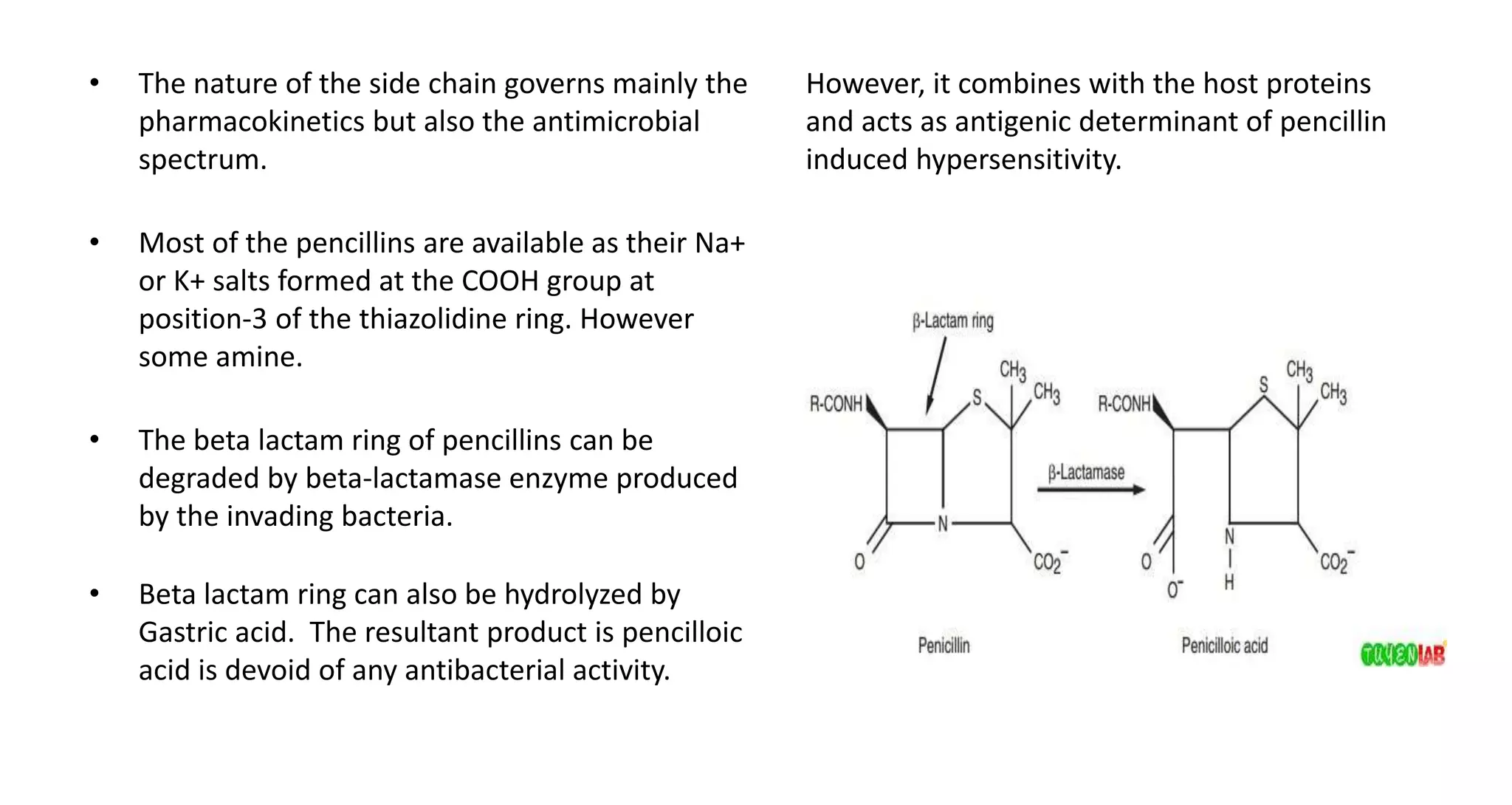
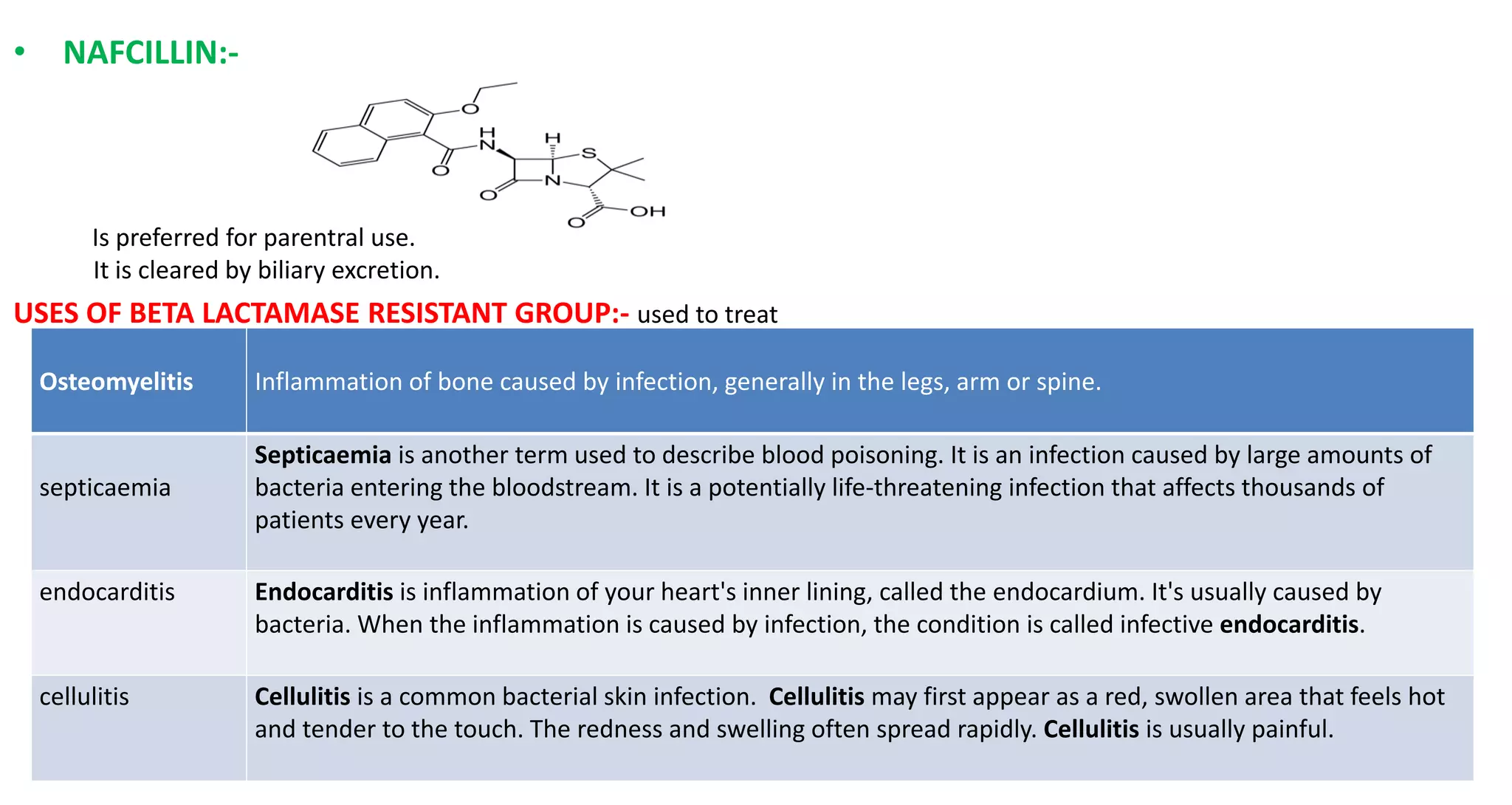
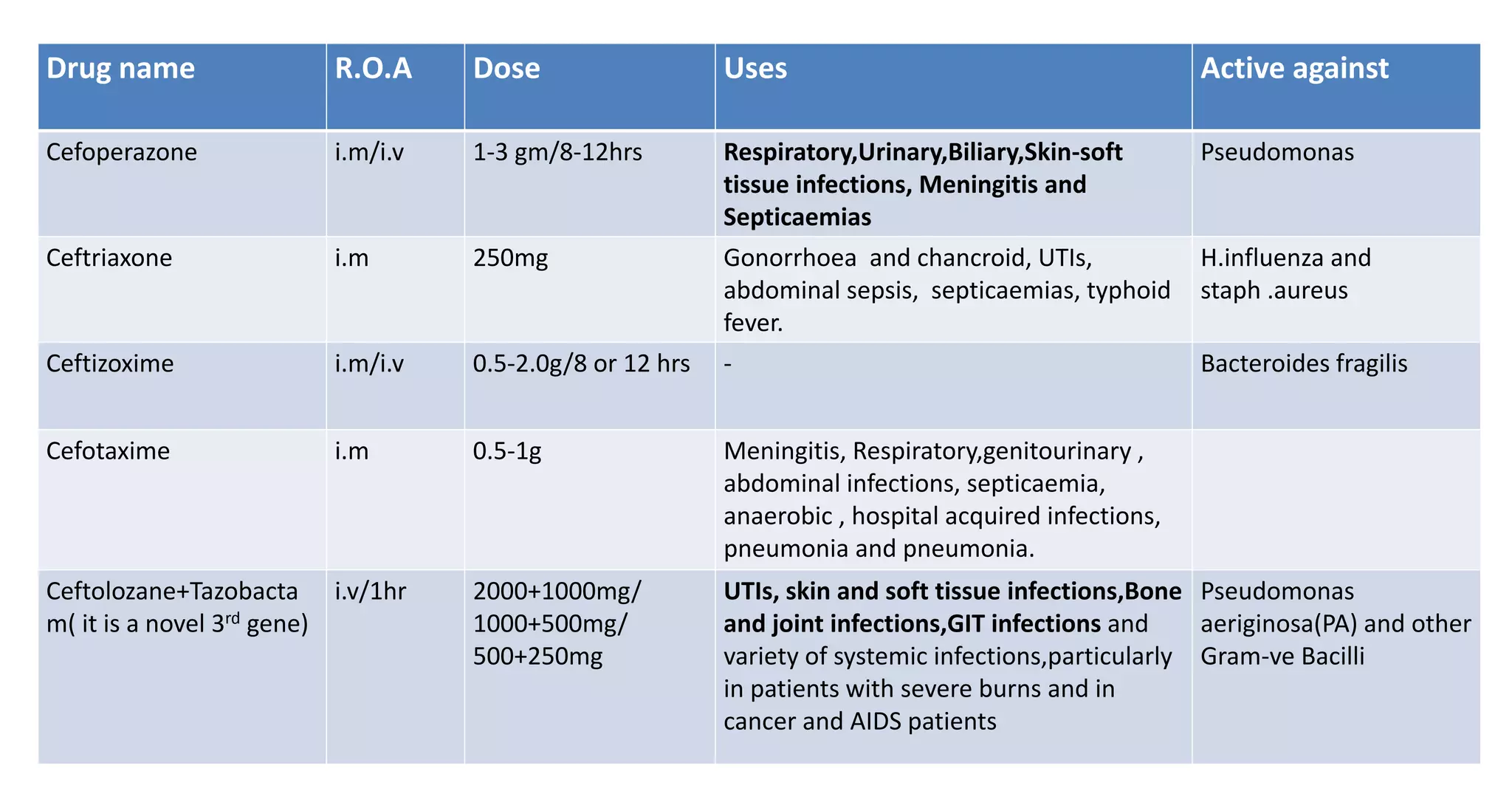
This document summarizes beta-lactam antibiotics, which are a class of antibiotics that contain a beta-lactam ring. It describes the structure and synthesis of bacterial cell walls, which are composed of peptidoglycan layers. Beta-lactam antibiotics such as penicillins inhibit bacterial cell wall synthesis by binding to penicillin-binding proteins. The document categorizes and describes different types of penicillins including natural penicillins, antistaphylococcal penicillins, and extended-spectrum penicillins. It provides details on mechanisms of action, pharmacokinetics, clinical uses and resistance mechanisms for various beta-lactam antibiotics.