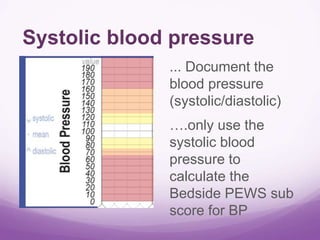
This document provides instructions for using the Bedside Pediatric Early Warning System (BPEWS). BPEWS involves assessing 7 critical indicators for pediatric patients, including heart rate, blood pressure, respiratory rate, oxygen saturation, oxygen therapy, respiratory effort, and capillary refill time. Scores are determined for each indicator and totaled to calculate an overall BPEWS score. BPEWS scores correspond to care recommendations including vital sign monitoring frequency, physician reviews, and nurse-to-patient ratios. The goal is to standardize pediatric early warning assessments and match patient care needs to their risk level.