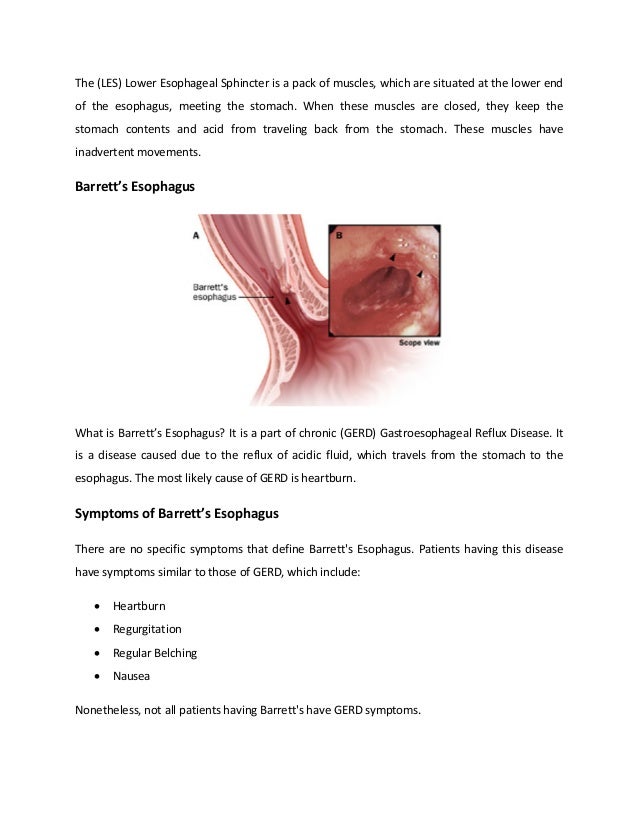
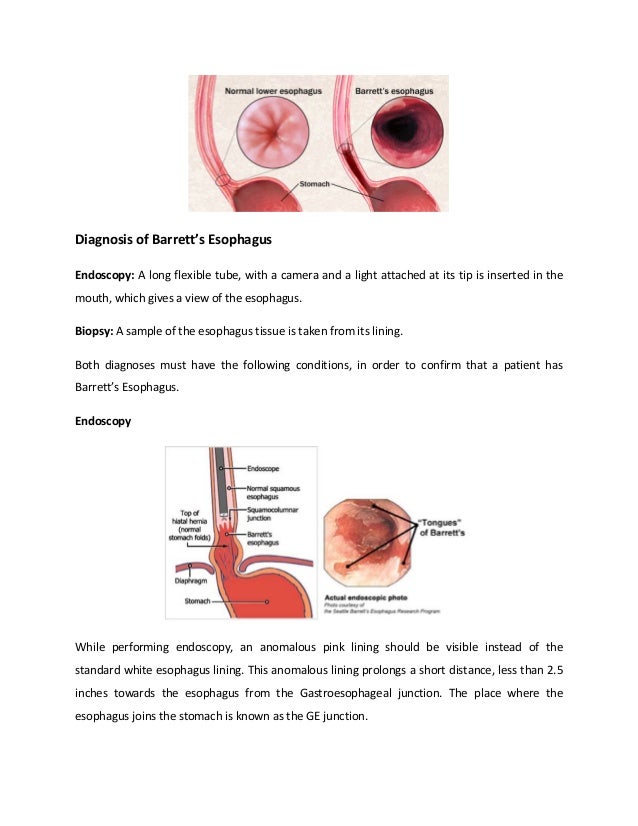
Barrett's esophagus is a condition where the lining of the esophagus is replaced by abnormal intestinal-type cells due to chronic acid reflux from the stomach. This occurs when stomach acid damages the normal esophageal lining over many years. The abnormal cells are pre-cancerous and increase the risk of developing esophageal adenocarcinoma. The main symptoms of Barrett's esophagus are heartburn and acid reflux. It is diagnosed through an endoscopy with biopsy to examine the abnormal cells under a microscope. The primary cause is gastroesophageal reflux disease which causes excessive stomach acid to back up into the esophagus.