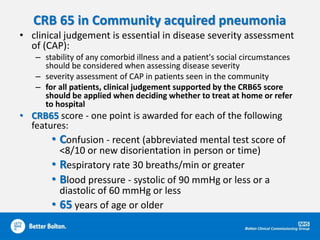
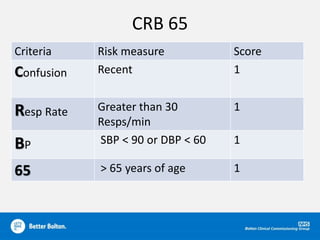
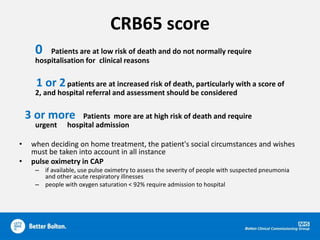
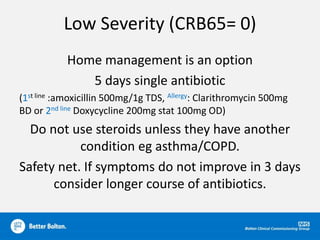
1. The document provides prescribing updates and recommendations for several medications and conditions, including pregabalin, vitamin D, the CRB-65 tool for pneumonia risk assessment, and SGLT2 inhibitors for diabetes.
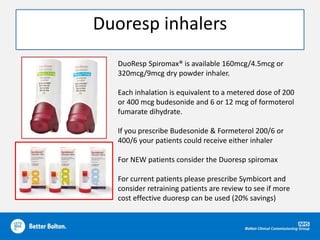
2. It recommends the Sirdupla and Duoresp inhalers as cheaper alternatives to other brands, and reviews options for switching patients between opioid formulations.
3. Specialist teams will take over prescribing of immunosuppressants for transplant patients, and the document provides guidance on items to include on the local "do not prescribe" list.