
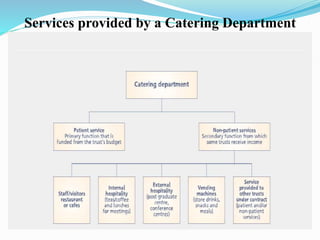



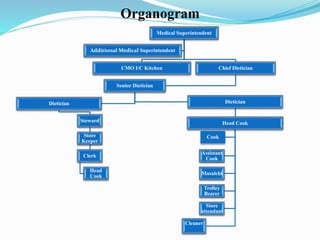
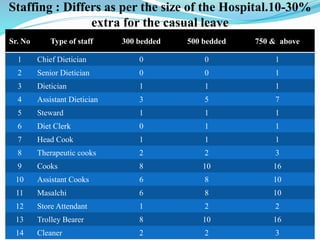

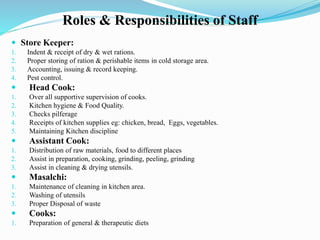
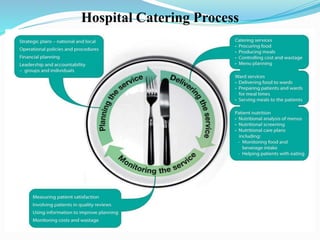




The document discusses hospital catering services. It provides details on core objectives and services of a catering department including menu planning, material management, costing, and food safety. It outlines the roles and responsibilities of catering staff. The document also discusses challenges around staffing and proposes remedial measures. Key performance indicators for evaluating catering services are presented. The conclusion emphasizes the importance of identifying patient nutritional needs, effective communication, and continual quality improvement.










































































![APPROACH TO FEVER IN PEDIATRICS[1].pptTT](https://cdn.slidesharecdn.com/ss_thumbnails/approachtofeverinpediatrics1-260125081456-d559e079-thumbnail.jpg?width=640&height=640&fit=bounds)

