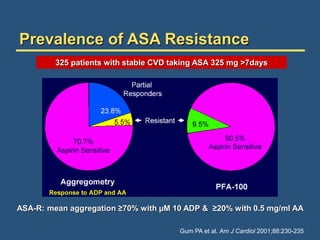
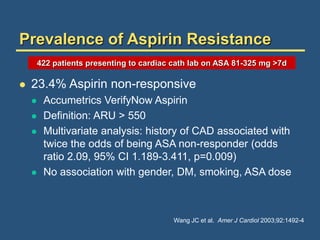
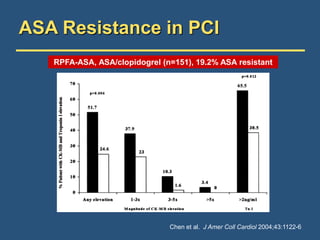
1) Aspirin resistance is defined as inadequate inhibition of platelet aggregation despite aspirin use and has a prevalence of 5-60% based on different tests.
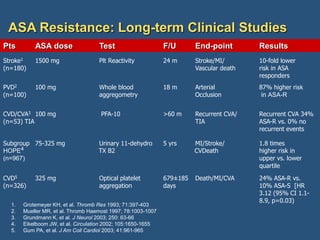
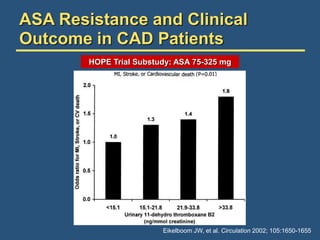
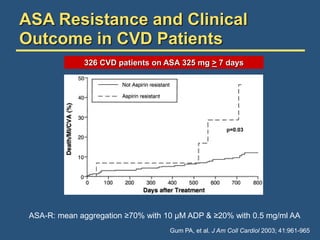
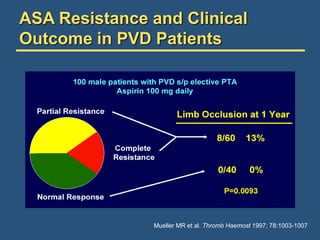
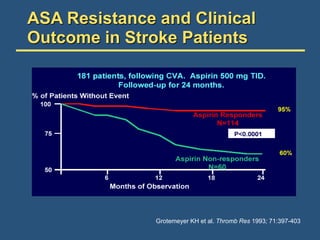
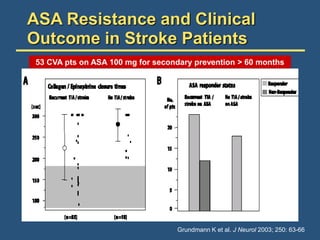
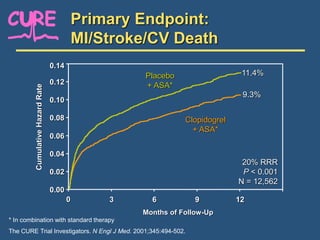
2) Several studies have found that aspirin resistance is associated with an increased risk of major adverse cardiovascular events such as heart attack, stroke, and death.
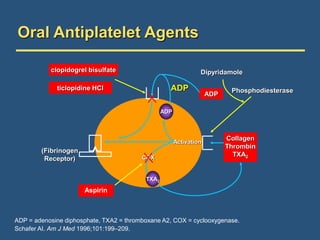
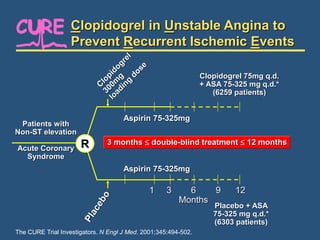
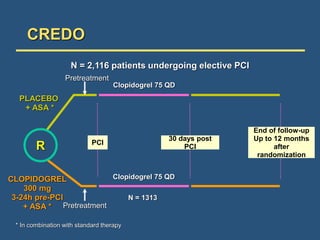
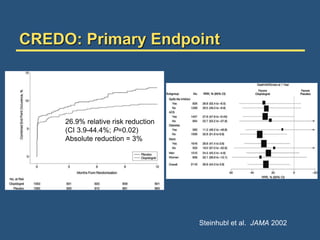
3) For patients who are aspirin resistant, management options include increasing the aspirin dose, adding other antiplatelet drugs like clopidogrel, and ensuring patient compliance with the medication regimen.









































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






