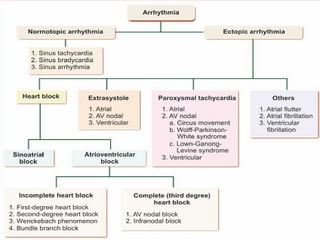
The document provides a comprehensive overview of cardiac arrhythmias, defining terms such as tachycardia, bradycardia, and various types of arrhythmias including ectopic and paroxysmal tachycardias. It discusses the physiological and pathological conditions leading to abnormal heart rhythms and describes the clinical applications, causes, and implications of various arrhythmias, including heart block and ectopic foci of excitation. Furthermore, it addresses the effects of ionic composition changes in the blood on heart function and associated ECG patterns.







![Dysrhythmia [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/dysrhythmiaautosaved-230617180733-e317f7a6-thumbnail.jpg?width=640&height=640&fit=bounds)

























































