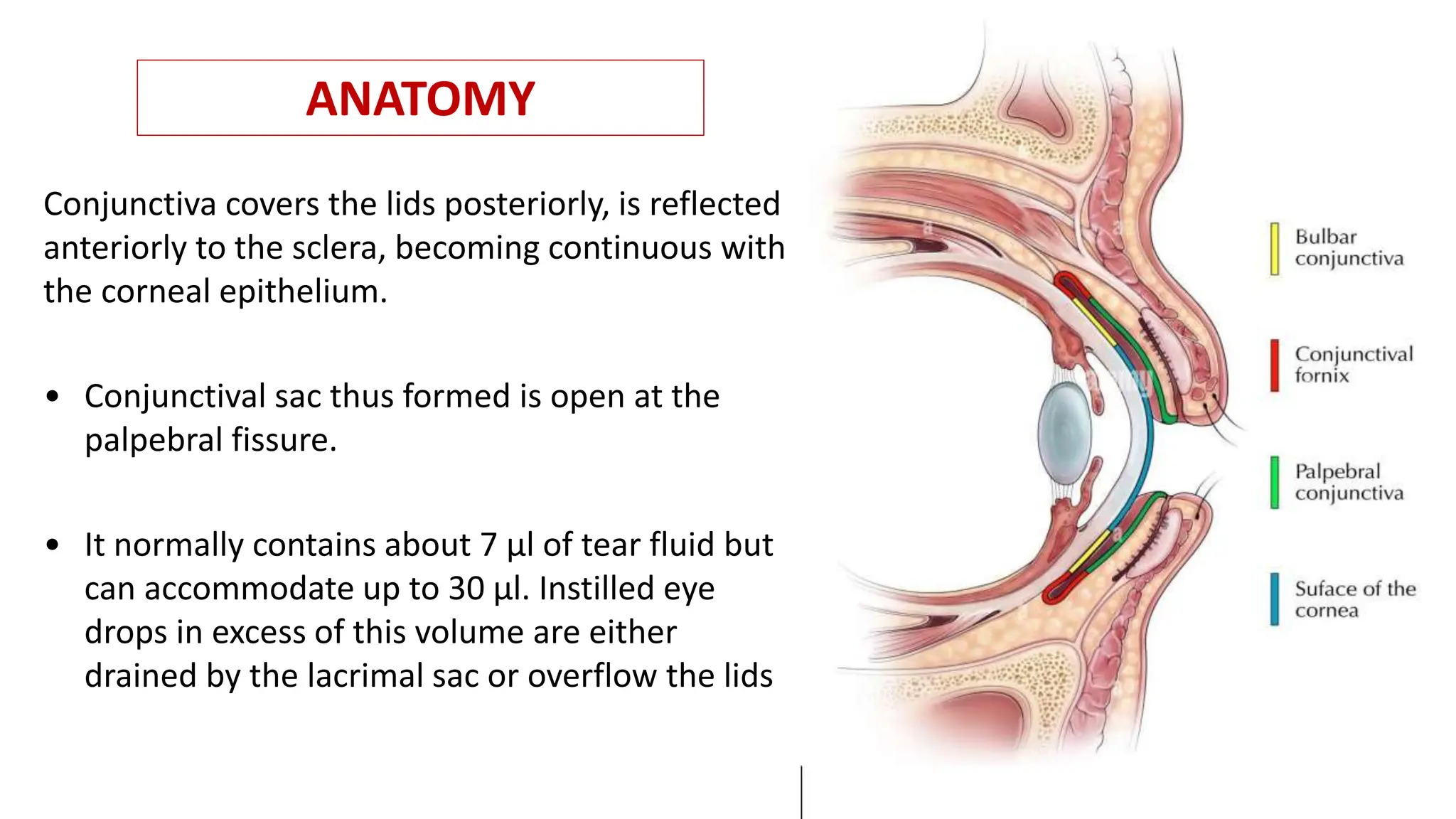
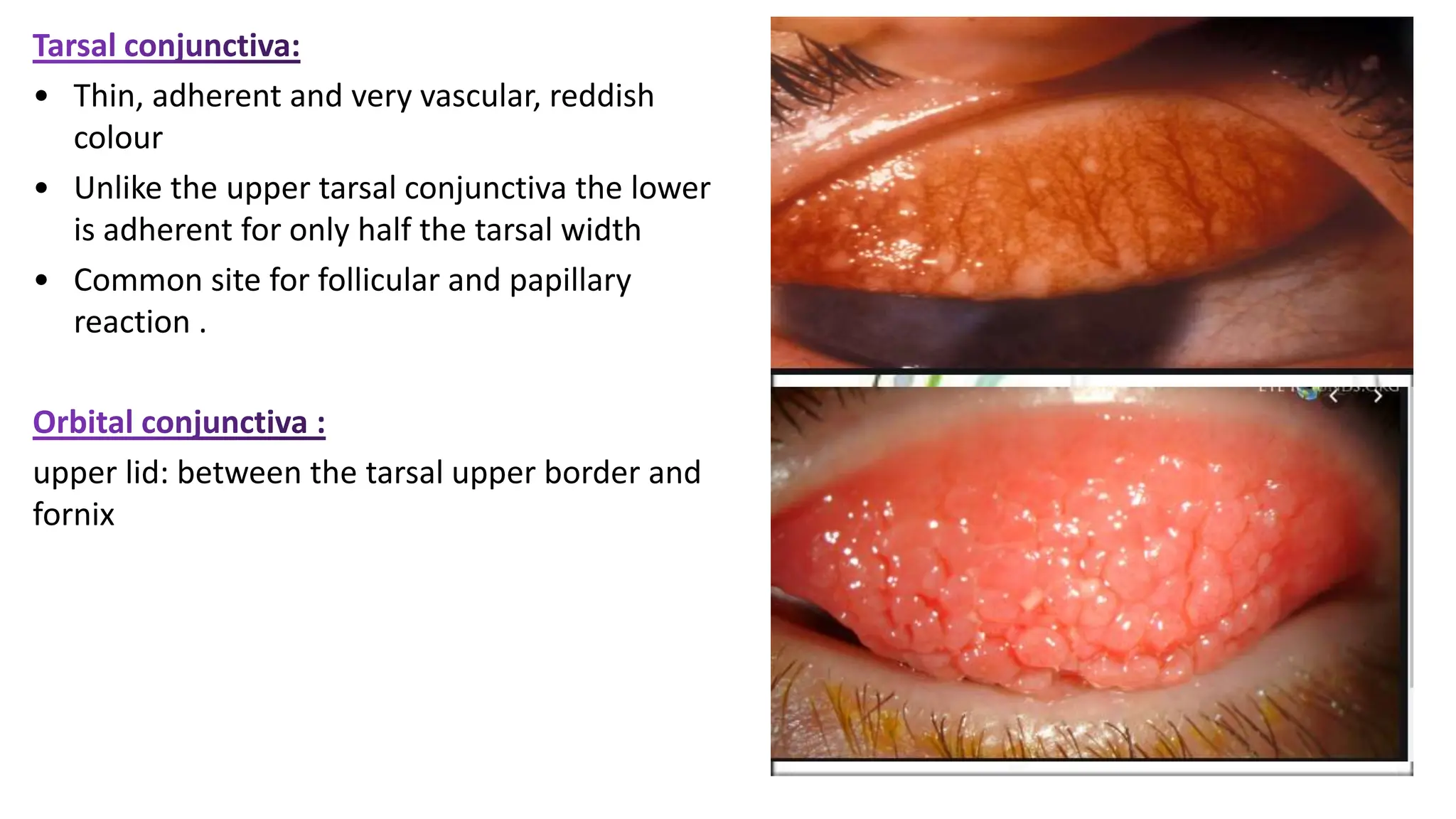
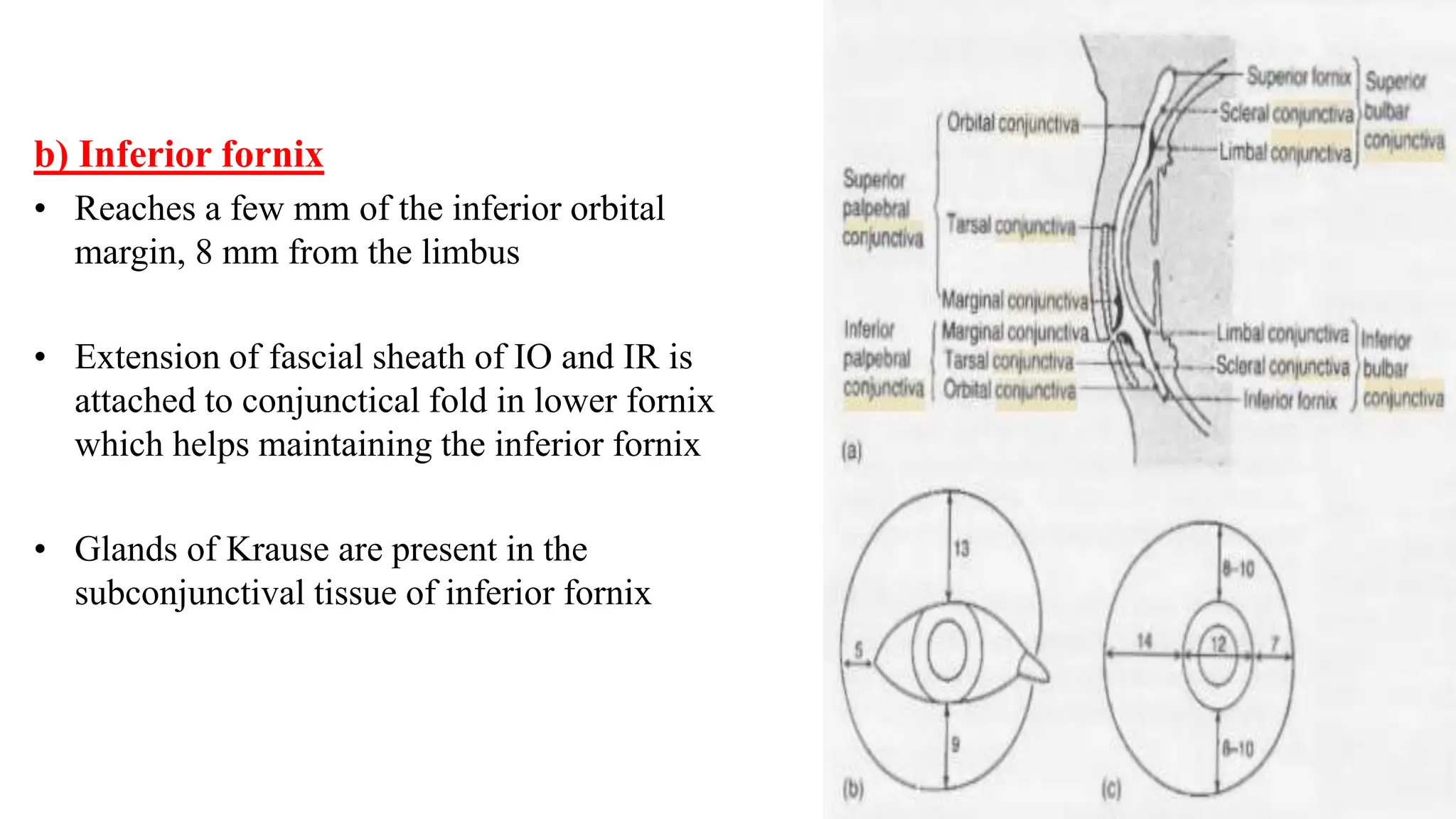
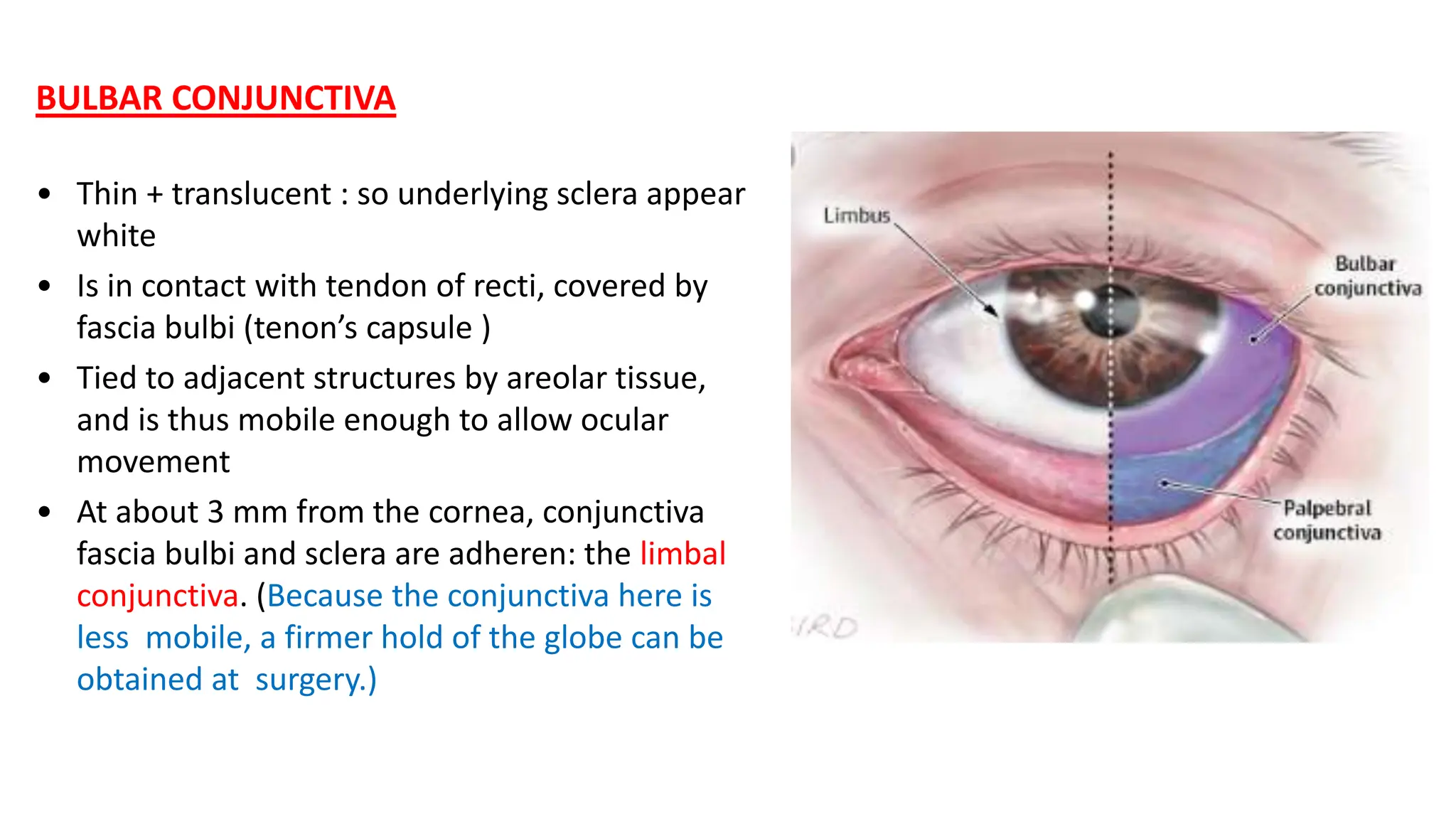
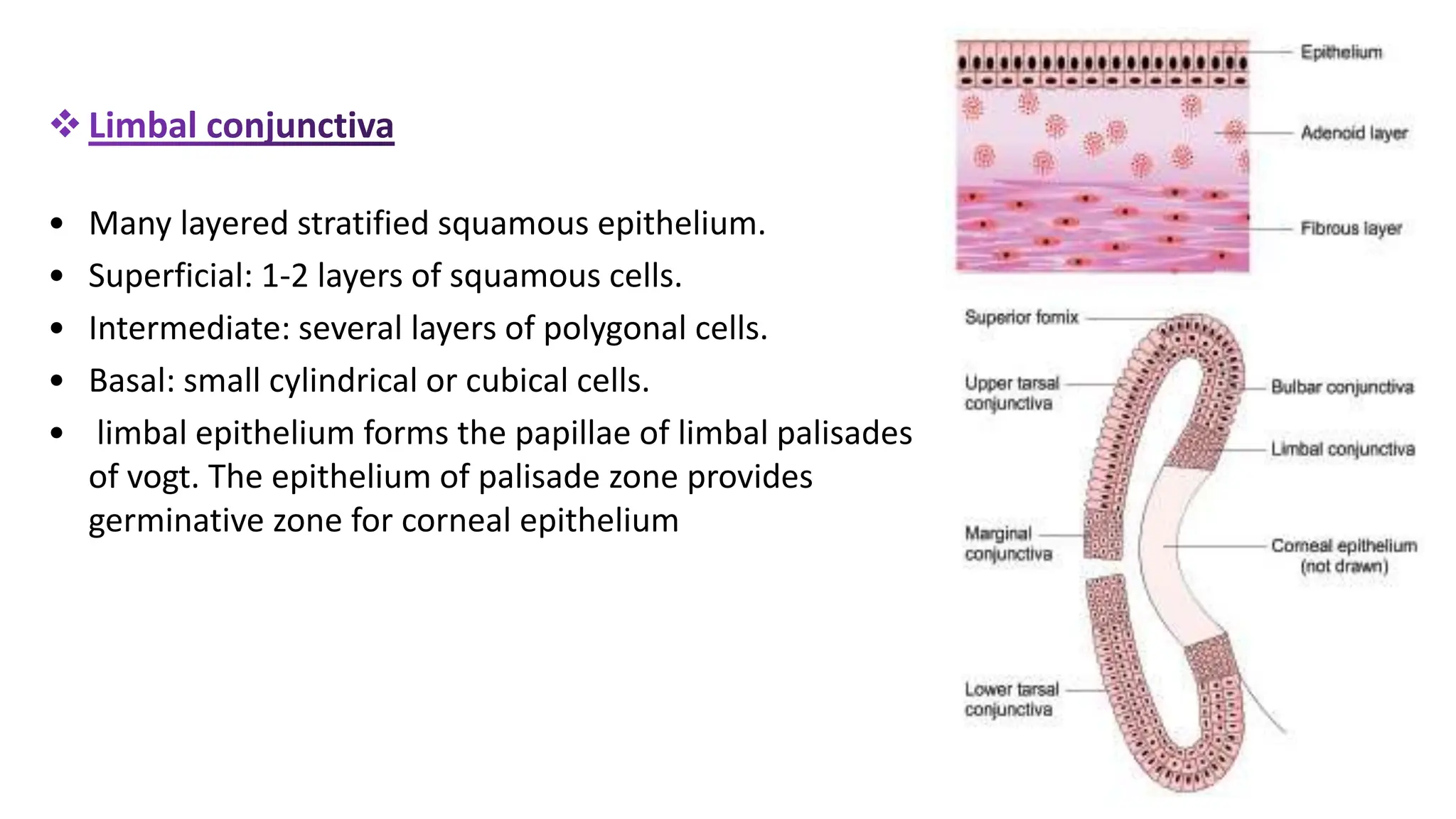
The conjunctiva covers the sclera and lines the eyelids. It has 3 layers - epithelium, adenoid layer containing lymphoid tissue, and fibrous layer. The conjunctiva secretes mucin via goblet cells and aqueous fluid via accessory lacrimal glands. It is highly vascular and innervated. Clinical signs of conjunctivitis include redness, discharge, membranes, follicles, papillae, and scarring. The conjunctiva plays a key role in tear film production and defense of the ocular surface.