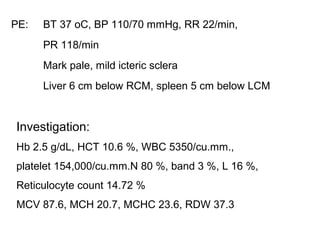
PE: BT 37oC, BP 110/70 mmHg, RR 22/min,
PR 118/min
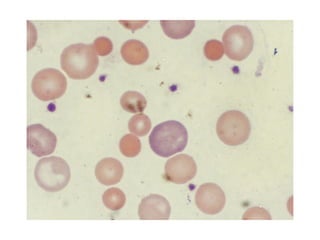
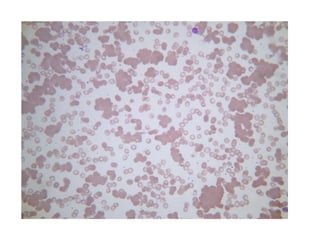
Mark pale, mild icteric sclera
Liver 6 cm below RCM, spleen 5 cm below LCM
Investigation:
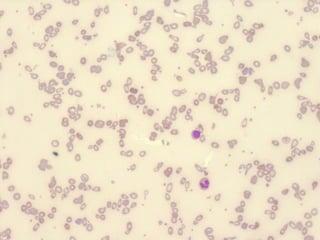
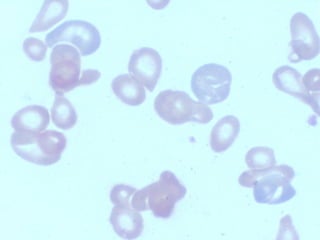
Hb 2.5 g/dL, HCT 10.6 %, WBC 5350/cu.mm.,
platelet 154,000/cu.mm.N 80 %, band 3 %, L 16 %,
Reticulocyte count 14.72 %
MCV 87.6, MCH 20.7, MCHC 23.6, RDW 37.3
8.
Chol 104, alb4, glob 3.5, TB 4.5, DB 0.7, ALT 23,
AST 28, AP 64
Hb typing EABart’sH [E 10%, F 0.7%]
Direct Coombs test – positive 3+
Indirect Coombs test – positive 4 +
Identify alloantibody – anti E
Red blood celltransfusionRed blood cell transfusion
Least incompatible blood
21.
Red blood celltransfusionRed blood cell transfusion
Patient should be tested for co-existing alloantibodies
(15-40 %)
Alloantibodies > autoantibodies cause major
transfusion reaction
Most patients tolerate even serologically incompatible
blood
Patient with symptoms of severe anemia

![Chol 104, alb 4, glob 3.5, TB 4.5, DB 0.7, ALT 23,
AST 28, AP 64
Hb typing EABart’sH [E 10%, F 0.7%]
Direct Coombs test – positive 3+
Indirect Coombs test – positive 4 +
Identify alloantibody – anti E](https://image.slidesharecdn.com/aiha-chittima-1258965695-phpapp01/85/AIHA-8-320.jpg)