Adverse Drug Reaction
“Anyresponse to drug, which is noxious &
unintended which occurs at doses normally
used for treatment, prophylaxis, diagnosis,
or modification of physiological function.”
2.
Adverse Drug Event
“Anyuntoward medical occurrence that
may present during treatment with
medicine but does not necessary have
causal relationship with the treatment. “
3.
Serious adverse event
Anyuntoward medical occurrence,
that at any dose;
Results in death
Requires hospitalization or prolongation of existing
hospitalization
Results in persistent significant disability or incapacity
Requires intervention to prevent permanent injury
From theearliest times, pharmaceutical
formulations have been recognized as
being potentially dangerous.
Everytime we give a drug we take a risk
Public and professional concern about
these matters first arose in the late 19th
century.
In 1922, there was an enquiry into the
JAUNDICE associated with the use of
SALVARSAN, an organic arsenical used
6.
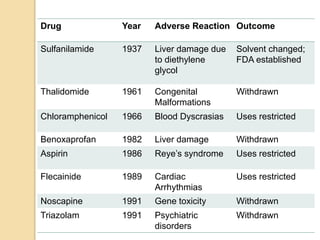
In 1937in USA,
107 people died from taking
an Elixir Of Sulfalinamide
that contained the Solvent
Di-ethylene Glycol
This led to establishment of FOOD AND DRUG
ADMINISTRATION (FDA), which was given the
task of enquiring into the safety of new drugs
before allowing them to be marketed
7.
In 1961,it was reported in West
Germany that there was an outbreak of
PHOCOMELIA (hypoplastic and
aplastic limb deformities) in the new
born babies.
8.
The ThalidomideIncident led to
development of a much more
sophisticated approach to preclinical
testing & clinical evaluation of drugs
before marketing, & greatly increased
awareness of adverse effect of
drugs and methods of detecting
them.
Incidence
Hospital in-patients:10-20%
Deaths inhospital in-patients: 0.3-3%
Hospital admissions: 0.3-5%
Worldwide – ADRs: 6th leading cause
of
death
US and Canada – ADRs: 4th leading
cause of death
11.
Why incidence ismore ?
1) Ever-increasing number of new drugs
in the market
2) Number of drugs prescribed are high
3) Medication errors
4) Lack of awareness of a system for
reporting ADR’S
12.
Common causes
Failingto take the correct dose at the
correct times
Overdosing
Allergies to chemical components of
the medicine
Combining the medicine with alcohol
Taking other drugs or preparations
that interact with the medicine
13.
Factors affecting AdverseDrug
Reactions :
Age
Genetic influences
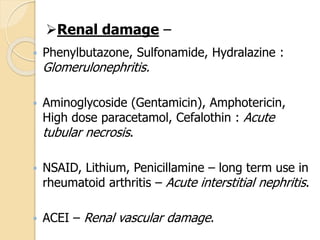
Concurrent diseases (Renal, Liver,
Cardiac)
Previous adverse drug reactions
Compliance with dosing regimen
Total number of medications
Misc. (diet, smoking, environmental
exposure)
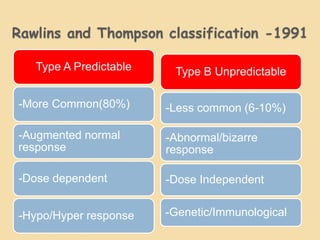
Rawlins and Thompsonclassification -1991
Type A Predictable
-More Common(80%)
-Augmented normal
response
-Dose dependent
-Hypo/Hyper response
Type B Unpredictable
-Less common (6-10%)
-Abnormal/bizarre
response
-Dose Independent
-Genetic/Immunological
16.
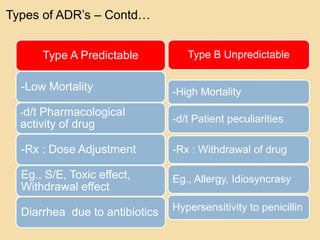
Type A Predictable
-LowMortality
-d/t Pharmacological
activity of drug
-Rx : Dose Adjustment
Eg., S/E, Toxic effect,
Withdrawal effect
Diarrhea due to antibiotics
Type B Unpredictable
-High Mortality
-d/t Patient peculiarities
-Rx : Withdrawal of drug
Eg., Allergy, Idiosyncrasy
Hypersensitivity to penicillin
Types of ADR’s – Contd…
17.
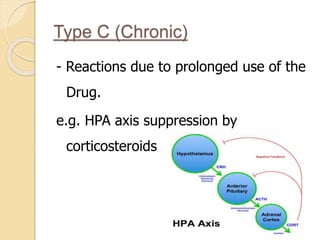
Type C (Chronic)
-Reactions due to prolonged use of the
Drug.
e.g. HPA axis suppression by
corticosteroids
18.
Type D (Delayed)
•Occuring years after the treatment
• Can be due to accumulation
E.g : Teratogenisis
19.
Type E (Endof use)
• Occur on withdrawal especially when
drug is stopped abruptly
E.g.
• Precipitation of MI by β blocker
withdrawl
20.
Type F (Failureof drug)
Underdosing of medications
Drug interactions
Eg: OCP failure
21.
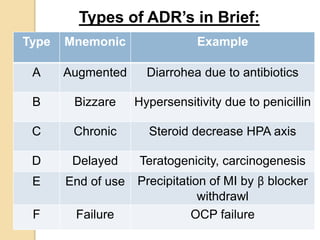
Type Mnemonic Example
AAugmented Diarrohea due to antibiotics
B Bizzare Hypersensitivity due to penicillin
C Chronic Steroid decrease HPA axis
D Delayed Teratogenicity, carcinogenesis
E End of use Precipitation of MI by β blocker
withdrawl
F Failure OCP failure
Types of ADR’s in Brief:
22.
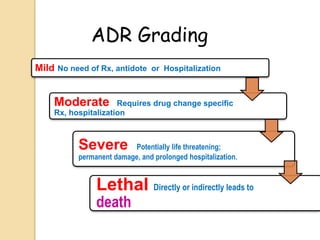
Mild No needof Rx, antidote or Hospitalization
Moderate Requires drug change specific
Rx, hospitalization
Severe Potentially life threatening;
permanent damage, and prolonged hospitalization.
Lethal Directly or indirectly leads to
death
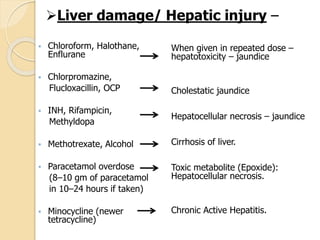
ADR Grading
“Unwanted but oftenunavoidable
pharmacodynamic effects of a drug at
therapeutic doses”
As Extension of therapeutic effect
Atropine - dry mouth
As distinctly different effect
Promethazine – Sedation.
Side effect exploited for therapeutic use
Codeine – Diarrhoea
1) SIDE EFFECTS
25.
“Indirect consequence ofPrimary action of
a drug”
Eg:
- Tetracycline : Superinfection
- Corticosteroids : Activation of latent
Tuberculosis
2)SECONDARY EFFECTS
26.
“Excessive pharmacological actionof a
drug due to over dosage or prolonged
use”
Eg:
- Functional alteration : Atropine - delirium
- Drug induced tissue damage : PCM –
Hepatic necrosis
- Extension of therapeutic effect :
Barbiturates – Coma
- Another action : Morphine – Respiratory
failure
3) TOXIC EFFECTS
27.
“Appearance of characteristictoxic
effects of a drug at therapeutic doses”
Eg.,
Triflupromazine (single dose) - Muscular
dystonia
Carbamazepine (few doses)– Ataxia
Chloroquine (single dose) - Vomiting
4)INTOLERANCE
28.
Unusual responseto a drug due to genetic
abnormality.
Drug interacts with some unique feature of the
individual, not found in majority subjects, and
produces the uncharacteristic reaction.
E.g.
Isoniazid: N-Acetylation affects the metabolism of
isoniazid
Slow N-Acetylation: Isoniazid is more likely to cause
peripheral neuritis
Fast N-Acetylation: cause hepatotoxicity in this group
5) IDIOSYNCRASY
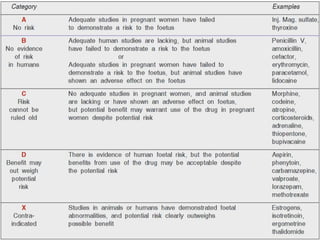
US FDAgraded documentation of risk for
causing birth defects into five categories
ABCDX
Avoid all drugs unless benefits
outweighs the risks
Eg: Phenytoin – cleft palate
Valproate – Spina bifida
Aspirin – premature closure of ductus
arteriosus
7)TERATOGENECITY
32.
8) Drug Allergy
◦Acquired, altered reaction of the body to
drug.
◦ Immunologically mediated reaction.
◦ occur even with much smaller doses
◦ Also called Drug hypersensitivity
◦ Not genetic, not occur in all
◦ Occurs on re-exposure
◦ E.g. penicillin→1st time →stimulate
antibody →Ag-Ab reaction →allergy
◦ Chief organ: Skin, respiratory tract, GIT,
Blood & blood vessels
33.
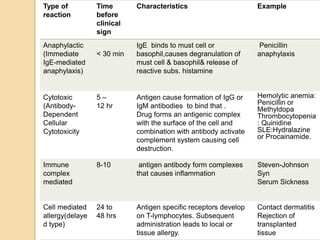
Type of
reaction
Time
before
clinical
sign
Characteristics Example
Anaphylactic
(Immediate
IgE-mediated
anaphylaxis)
<30 min
IgE binds to must cell or
basophil,causes degranulation of
must cell & basophil& release of
reactive subs. histamine
Penicillin
anaphylaxis
Cytotoxic
(Antibody-
Dependent
Cellular
Cytotoxicity
5 –
12 hr
Antigen cause formation of IgG or
IgM antibodies to bind that .
Drug forms an antigenic complex
with the surface of the cell and
combination with antibody activate
complement system causing cell
destruction.
Hemolytic anemia:
Penicillin or
Methyldopa
Thrombocytopenia
: Quinidine
SLE:Hydralazine
or Procainamide.
Immune
complex
mediated
8-10 antigen antibody form complexes
that causes inflammation
Steven-Johnson
Syn
Serum Sickness
Cell mediated
allergy(delaye
d type)
24 to
48 hrs
Antigen specific receptors develop
on T-lymphocytes. Subsequent
administration leads to local or
tissue allergy.
Contact dermatitis
Rejection of
transplanted
tissue
34.
9)Tachyphylaxis
When responsivenessdiminishes rapidly after
administration of a drug, the response is said
to be subject to tachyphylaxis.
Tyramine can cause depletion of all NE
stores if we use it repeatedly at short
interval, resulting in tachyphylaxis.
35.
10) Drug dependence
Drugs capable of altering mood and feelings
are liable for repetitive use to derive euphoria,
withdrawal from reality, social adjustment, etc.
Psychological dependence: Individual
believes that optimal state of well being is
achieved only through the actions of the drug.
E.g. Opioids, Cocaine.
Physical dependence: Altered physiological
state produced by repeated administration of a
drug which necessitates the continued
presence of the drug to maintain physiological
equilibrium.
E.g. Opioids, Barbiturates, Alcohol,
36.
11) Mutagenicity andCarcinogenicity
Capacity of a drug to cause genetic defects and
cancer respectively.
Chemical carcinogenesis generally takes several
(10-40) years to develop.
Unpredictable
e.g.
Estrogen- Endometrial carcinoma.
OCP- Ca cervix, breast Ca
Iron S/C or I/M – blackening of area – increase
incidence of sarcoma (cause is unknown).
Anticancer drug.
Who can getan ADR?
Anyone who takes medicine
Differential diagnosis should
include the possibility of an
ADR if the patient is taking any
form of medication
43.
If symptoms,
Appears soonafter a new drug is
started
Appears after an increase in dose
Disappears when the drug is
stopped
Reappears when a drug is restarted
When To Report :
Pharmacovigilance
The science andactivities relating to
detection, assessment, understanding
& prevention of adverse effects or any
other drug related problem
- WHO 1972
Why Pharmacovigilance ?
Humanitarian concerns “First do no harm”
Reduce disease related economic loss
Check if drugs available in market fulfill
their intended role in society.
46.
ADR Monitoring inIndia
1980- Concept of Pharmacovigilance in India
1982- 5 Centers established by DCGI for
nationwide monitoring of ADR
1987- ICMR establishes many centers for
nationwide monitoring of ADR
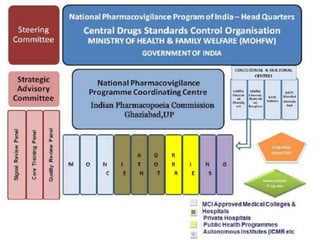
Nov. 2004- National Pharmacovigilance
programme was started consisting of national
centers, 2 zonal centers, 5 regional centers and 28
peripheral centers
48.
GMC,NAGPUR
Recognized indec.2012
Started reporting from 2013
No. of cases reported:
2013-77
2014-388
2015-347
2016-162
49.
Why is ADRMonitoring Needed?
Unreliability of pre-clinical studies
Limitations of pre-marketing phases of clinical
trial
Aggressive marketing strategies of
pharmaceutical companies
Changing physician and patient preference
Easy accessibility of drugs
50.
Limitations of pre-marketingphases
of clinical trial
Conducted in strictly controlled
conditions, in highly selected and
limited number of patients
Fails to detect rare and delayed ADRs
Do not provide data –
- In children, elderly patients,
pregnant/lactating women
- In patient suffering from other
disease
- In patient receiving other drugs
- On interpopulation difference
51.
Various reporting systemsare-
WHO international system(Uppsala
monitoring centre, Sweden)
US FDA "Med watch"
UK "Yellow card system"
PvPI under CDSCO, India
52.
• Doctors
• Dentists
•Nurses
• Pharmacists
Health care
professiona
ls
• Patients
• Consumers
• Relatives
Others
Who can report
??
53.
Problems in ADRreporting
Patient Related
(i) Cannot
recognize ADR
(ii) Recognize but
do not report
(iii) Illiteracy
Health proffesional
Related
(i) Cannot recognize ADR
(ii) Recognize but do not
report due to
- Lack of time
- Hesitancy
- Ignorance
- Fear of litigation
- Guilt
Causality Assessment
Routineprocedure in
Pharmacovigilance
Relationship of cause & effect
Most outcomes : multiple interacting
causes
Aim : to define contribution due to
drugs
Problems:
ADRs rarely specific
Diagnostic tests usually absent
Re challenge rarely ethically justified
58.
Causality Assessment Methods
Algorithmic:
Seriesof questions
Answers are weighted
Overall score determines causality
category
e.g. Naranjo’s scale
Probalistic:
Set of explicitly defined causality
categories
59.
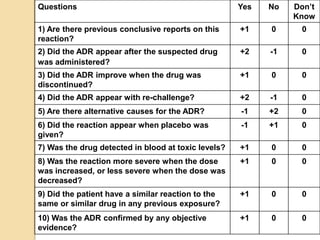
Questions Yes NoDon’t
Know
1) Are there previous conclusive reports on this
reaction?
+1 0 0
2) Did the ADR appear after the suspected drug
was administered?
+2 -1 0
3) Did the ADR improve when the drug was
discontinued?
+1 0 0
4) Did the ADR appear with re-challenge? +2 -1 0
5) Are there alternative causes for the ADR? -1 +2 0
6) Did the reaction appear when placebo was
given?
-1 +1 0
7) Was the drug detected in blood at toxic levels? +1 0 0
8) Was the reaction more severe when the dose
was increased, or less severe when the dose was
decreased?
+1 0 0
9) Did the patient have a similar reaction to the
same or similar drug in any previous exposure?
+1 0 0
10) Was the ADR confirmed by any objective
evidence?
+1 0 0
60.
The Naranjo ProbabilityScale
The score :-
≥ 9 = Definite
5-8 = Probable
1-4 = Possible
0 = Doubtful
Summary
Every drugwhich has an effect has an adverse
effect every time a drug is given risk is involved
For rational use of drug not only its clinical
indications are important but the knowledge of
adverse effects as well
Early detection of adverse effects and its
proper management can be life saving in many
situations
ADR Reporting (Pharmacovigilance) plays a
important role in the evolution and life history of
a drug