Download as PDF, PPTX
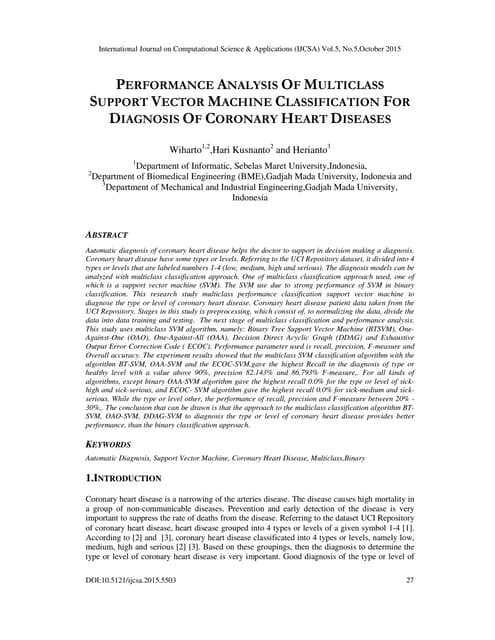
![Combining Neurodegenerative Characterization with Amyloid Burden Measurement Using an Early Frame Amyloid PET Multivariate Classifier
Matthews DC MS MM1, Lukic AS PhD1, Andrews RD MS1, Wernick MN PhD1,2, Strother SC, PhD1,3, Schmidt ME MD4 for the Alzheimer’s Disease Neuroimaging Initiative
1ADM Diagnostics LLC, Chicago, Illinois, USA, 2Medical Imaging Research Center, Illinois Institute of Technology, Chicago, Illinois, USA, 3Baycrest Hospital, Toronto, Ontario, Canada, 4Janssen Pharmaceutica, Beerse, Belgium
INTRODUCTION
OBJECTIVES
Measurement of amyloid burden provides important confirmation of
Alzheimer’s disease (AD) pathology for clinical trials and diagnosis.
However, many amyloid+ (Am+) early stage subjects do not worsen
clinically during the timeframe of a clinical trial, and a measure of
neurodegeneration that is predictive of clinical decline could provide a
useful adjunct to amyloid burden.
Previous studies have shown correspondence between perfusion
measured by the early amyloid frames following tracer injection and
FDG PET1,2. For example, Figure 1 shows the summed early frames of
an amyloid PET scan acquired in a subject, and the FDG PET scan
acquired at the same approximate time point.
RESULTS
REFERENCES AND ACKNOWLEDGEMENTS
DISCUSSION AND CONCLUSIONS
Figure 1. Summed early frames of 11C-PIB scan (left) and FDG scan
(right) in same ADNI 1 subject, similar time point
METHODS
Table 1. Subject characteristics
Data used in this study were obtained from the ADNI database (www.adni-info.org). As
such, ADNI investigators contributed to the design and implementation of ADNI and/or
provided data but did not participate in analysis or writing of this report.
This work was supported in part by SBIR grant -IIP-1256638 from the National Science
Foundation and in part by Janssen Research and Development.
For further information:
Dawn C. Matthews, ADMdx
dmatthews@admdx.com
[1] Hsiao IT et al, Eur J Nucl Med Mol Im, 2012
[2] Rostomian AH et al, J Nucl Med, 2011
[3] Lin KJ et al, Eur J Nucl Med Mol Im, 2016
[4] Matthews DC et al, Alz & Dem, Suppl, 2015
[5] Joshi A et al, Neuroimage, 2009
[6] Ashburner J, Neuroimage, 2007
[7] Strother SC et al, 19th Conf Comp
Statistics, 2010
[8] Strother SC et al, Neuroimage, 2002
However, studies of EFA have also found limitations in measurement
sensitivity, particularly in early disease stages1,3. Multivariate machine
learning approaches can offer a sensitive means for detection of
disease related changes. Using these methods and 166 ADNI subjects,
we have previously developed an AD Progression classifier that assigns
a numeric score to a subject’s FDG PET scan reflecting the degree to
which they express a pattern associated with progressing AD. This
score is predictive of subsequent cognitive decline in populations
ranging from Normal Am+ subjects to AD4. In this work, we applied the
same approach to determine whether we could develop a predictive
classifier using EFA.
• To evaluate early frame amyloid (EFA) as measure of AD-related
neurodegeneration, using multivariate machine learning
• To examine the correlation between EFA classifier scores and clinical
endpoints
• To understand similarities and differences between EFA vs. FDG
signal
• To assess the feasibility of using EFA for stratification and enrichment
One hundred-seven ADNI2 subjects were identified who had early
frame amyloid scans that passed quality control. For each scan,
timeframes for the first six minutes were motion corrected, summed,
smoothed to a common resolution5 and spatially warped to a common
template using the DARTEL algorithm6 in SPM8 (VBM8). Sixty-three
subjects were selected for five classifier training classes based upon
amyloid status using late timeframe SUVR and clinical diagnosis: 10 NL
amyloid-negative(-), 19 subjective memory complaints (SMC)-, 11
NL/SMC+, 9 MCI+, and 14 AD+ .
Using the NPAIRS framework7,8 implemented in our PipelineMAX™
software pipeline, Principal Component Analysis (PCA) was performed,
followed by determination of an optimized set of Canonical Variates
(CVs) through iterative resampling and calculation of reproducibility and
prediction metrics. Leave-One-Out testing was performed for validation
and the remaining scans not used in training were also scored.
EFA classification was compared to that of a FDG PET classifier
developed using the FDG scans of the same subjects at the same visit.
In addition, EFA scores were compared to the scores of the subjects’
FDG scans using our previously developed FDG AD Progression
classifier. Score distributions by diagnostic class and correlations with
clinical endpoints were compared. In addition, intensity values for
several regions including those relevant to AD and those typically used
as reference values for Standardized Uptake Value Ratio (SUVR)
measures were compared between EFA and FDG.
The EFA classifier produced a primary pattern (CV1, Figure 2 a,b)
corresponding to disease staging and characterized by reduced signal
in regions typical of neurodegeneration and reduced glucose
metabolism in AD. This pattern corresponded closely with that of the
classifier developed using FDG PET scans from the same subjects and
same visits as available (Figure 2 c,d), and with the previously
developed FDG AD Progression classifier. Leave One Out test scores of
the EFA classifier correlated strongly with FDG classifier test scores (R-
squareds = 0.81, Figure 2 e,f). The combined NL-SMC- class differed
from NL-SMC+ and MCI+ classes with both EFA (p<0.04, p<0.004) and
FDG (p<0.02, p<0.0004). The difference between MCI and AD scores
was consistent with the clinical difference (see Table 1).
Region
Difference (EFA - FDG) / FDG
NL- NL+ MCI+ AD+
Middle frontal -11% -6% -7% -3%
Superior frontal -9% -6% -7% -3%
Posterior Cingulate -9% -10% -6% -3%
Angular -9% -6% -6% 1%
Middle occipital -8% -7% -7% -5%
Inferior parietal -7% -3% -5% -2%
Inferior temporal -5% -3% -4% 0%
Supplemental Motor -4% -1% -2% -3%
Middle temporal -4% -3% -3% 1%
Putamen -2% -4% -3% -3%
Superior temporal 0% 0% 0% -1%
Anterior cingulate 2% 1% 4% 4%
Subcortical White 3% 2% 3% 2%
Cerebellar cortex 10% 10% 10% 7%
Hippocampus 11% 10% 10% 7%
Amygdala 13% 13% 12% 10%
Thalamus 15% 15% 15% 14%
Pons 28% 27% 24% 25%
NL includes NL and SMC; MCI = EMCI and LMCI
• A multivariate machine learning classifier derived from EFA produces
a pattern reflecting AD progression and subject scores reflecting
pattern expression that are highly correlated with those produced
using FDG PET data.
• It is feasible to develop a predictive EFA classifier for disease
detection and clinical trial enrichment that is sensitive even to very
early changes in cognitively normal Am+ subjects.
• EFA images show lower signal intensity than FDG in cortical regions
affected in AD, but higher intensity in certain other regions including
thalamus, cerebellum, and pons; these differences are addressed
through modality specific classifier development.
• The ability to detect neurodegenerative status and progression using
EFA can provide an important adjunct to amyloid burden
measurement without requiring an additional PET scan.
Figure 2. Mean CV1 scores (bars=SEM) by training group generated
during independent Leave-One-Out (a) EFA classifier scoring of summed
first six minute scans, and (b) FDG classifier scoring of FDG scans for the
same subjects and visit where available. Eigenimages associated with the
primary CVs for the (b) EFA and (c) FDG classifiers. Correlation plots
between (e) EFA and FDG classifier scores, and (f) EFA vs. FDG AD
Progression classifier scores for all subjects including those not used in
training.
In region of interest
analyses, EFA scans had
lower cortical signal than
FDG in most regions, but
not uniformly. In contrast,
EFA scans had higher
signal in cerebellum,
pons, and thalamus –
regions that are typically
preserved in AD and
used as reference
regions. The overall
effect is reduced
sensitivity in detecting
neurodegeneration when
using standard SUVR
approaches.
Table 2. Region of interest
differences between EFA
and FDG.
Figure 3. Regional
differences between EFA
and FDG. Lower signal can
be observed in the cortical
regions of the EFA scan,
but higher signal in
cerebellum and subcortical
regions.
Despite lower dynamic range between some cortical regions and typical
reference regions, the EFA-trained multivariate classifier was able to
achieve similar performance to FDG. Figure 4 illustrates the difference
between using EFA SUVRs referenced to typical reference regions
(pons, cerebellum, whole brain, Figure 4a, b, c) vs. the EFA CV1 score
(Figure 4d) in differentiating disease stages. EFA CV1 effect sizes
exceeded those of the EFA SUVRs.
Within the 34 Am+ subjects, EFA CV1 scores correlated significantly
with clinical endpoints at baseline with R2 values of 0.35 for MMSE, 0.37
for CDR-sb, and 0.52 for ADAS-cog 13. This compared to values of
0.57, 0.62, and 0.79, respectively, for the FDG classifier developed
using the same subjects.
Figure 4. Comparison of EFA region of interest values and CV1 score for
NL-, NL+, EMCI+, LMCI+, and AD+ subjects](https://image.slidesharecdn.com/d318daa1-00d8-48bd-8e65-a29bf11d8061-160802232825/85/ADMdx_AAIC_2016_EFA_Neurodegeneration_Poster-1-320.jpg)

This study developed a machine learning classifier to analyze early frame amyloid PET scans and measure neurodegeneration related to Alzheimer's disease. The classifier produced scores that strongly correlated with scores from an FDG PET classifier, indicating it can detect disease progression. Early frame amyloid scans had lower cortical but higher subcortical signals compared to FDG PET. Nonetheless, the amyloid PET classifier achieved similar performance to FDG PET at differentiating disease stages. This suggests early frame amyloid PET can provide a measure of neurodegeneration without an additional scan, useful for clinical trials and diagnosis.
































![Mobile Automation Meetup Presentation [English]](https://cdn.slidesharecdn.com/ss_thumbnails/mobileautomationmeetuppresentation-english-150430163752-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)




























