This document provides an overview of acute pancreatitis including:
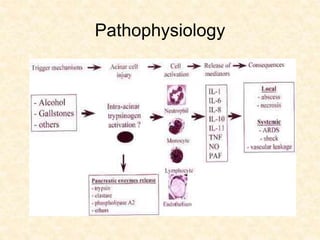
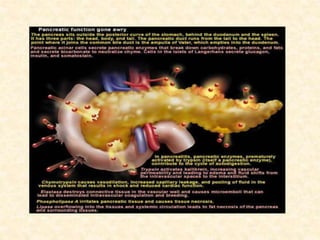
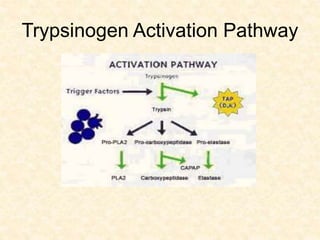
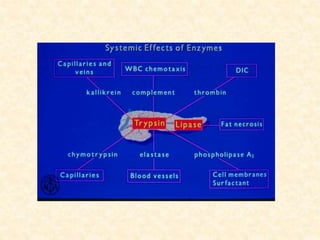
- The pathophysiology of premature activation of digestive enzymes within the pancreas leading to autodigestion.
- Common etiologies like gallstones, alcohol use, and hypertriglyceridemia.
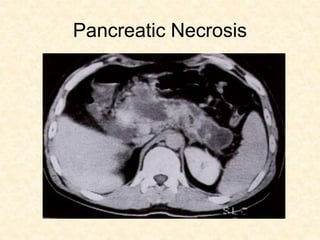
- Diagnosis through clinical signs/symptoms confirmed with lab tests like serum amylase and lipase levels or imaging like CT.
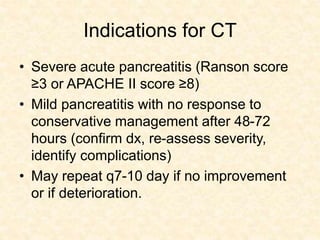
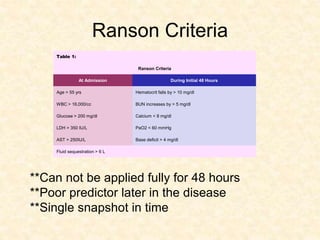
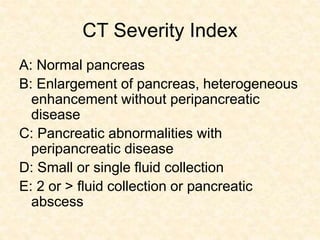
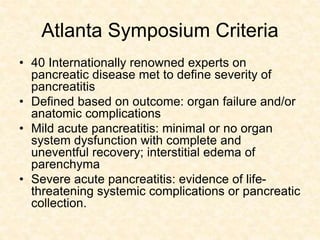
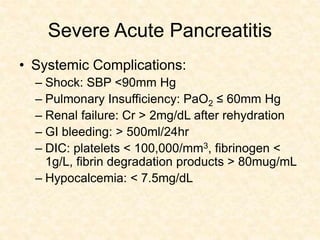
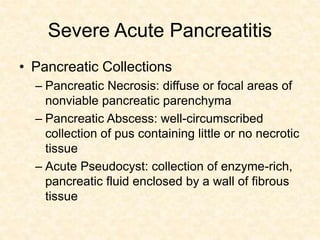
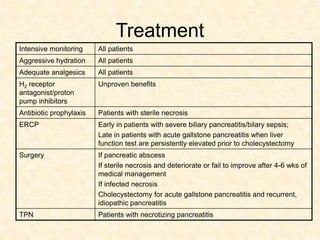
- Determining severity using criteria like Ranson score, APACHE II score, or evidence of organ failure/necrosis on CT.
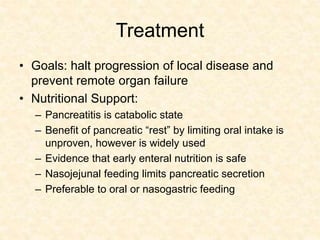
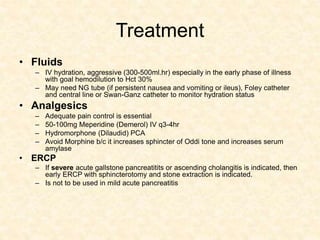
- Goals of treatment include halting disease progression, preventing organ failure through aggressive hydration and nutritional support, adequate pain control, and ERCP for severe gall




























![Acute pancreatitis [Autosaved].pptx surgery](https://cdn.slidesharecdn.com/ss_thumbnails/acutepancreatitisautosaved-240829144740-b197e85a-thumbnail.jpg?width=640&height=640&fit=bounds)








![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)












