For a diagnosed asthmatic patient presenting with breathlessness, the initial treatment would involve administering high doses of a rapid-acting inhaled bronchodilator like salbutamol every 20 minutes for the first hour. If the patient does not see adequate improvement, ipratropium bromide would be added. Systemic corticosteroids like prednisolone would also be prescribed if the exacerbation is severe or not responding to initial bronchodilator therapy, to reduce inflammation and control the attack.



![Acute asthma Symptoms
• Increased Breathlessness / Dysponea
[Difficulty in breathing]
• Increased Wheezing
[Whistling sound while exhaling]
• Increased Cough
[Often at night or after some exertion]
• Chest Tightness](https://image.slidesharecdn.com/acuteasthmappt-230107072745-2fe21f3d/75/Acute-Asthma-PPT-ppt-4-2048.jpg)
![Acute Asthma Signs
• Inability to complete a sentence
• Tachycardia [rapid heart beats]
• Tachypnea [rapid breathing]
• Accessory respiratory muscle use [around neck]
• Excessive sweating
• Cyanosis [blue discoloration of skin, lips in acute
severe cases]](https://image.slidesharecdn.com/acuteasthmappt-230107072745-2fe21f3d/75/Acute-Asthma-PPT-ppt-5-2048.jpg)

![Symptoms Mild- Moderate Severe- life threatening
Breathless On walking or talking At rest
Talks in Sentences / Phrases Words/
Unable to speak
Accessory muscles Usually not Usually
Central Cyanosis Absent Likely to be present
SaO2
[as measured by pulse
oximeter]
91-95%
OR
> 95%
< 90%
Pulse
rate
Adults <100-120 / min > 120 / min
Children <100-200 / min > 200 / min
Acute asthma classification
Refer to hospital
any patient with
features of
acute severe to life
threatening asthma](https://image.slidesharecdn.com/acuteasthmappt-230107072745-2fe21f3d/75/Acute-Asthma-PPT-ppt-7-2048.jpg)














![Management of mild / moderate
acute asthma
After brief history* and physical
examination…
*Rule out beta blocker or NSAID [aspirin] use, check for exposure
to strong trigger](https://image.slidesharecdn.com/acuteasthmappt-230107072745-2fe21f3d/75/Acute-Asthma-PPT-ppt-23-2048.jpg)

![Rapid Acting Bronchodilators
• Treatment should also be titrated depending upon the
individual patient response.
• No evidence to support the routine use of IV beta2
agonists.
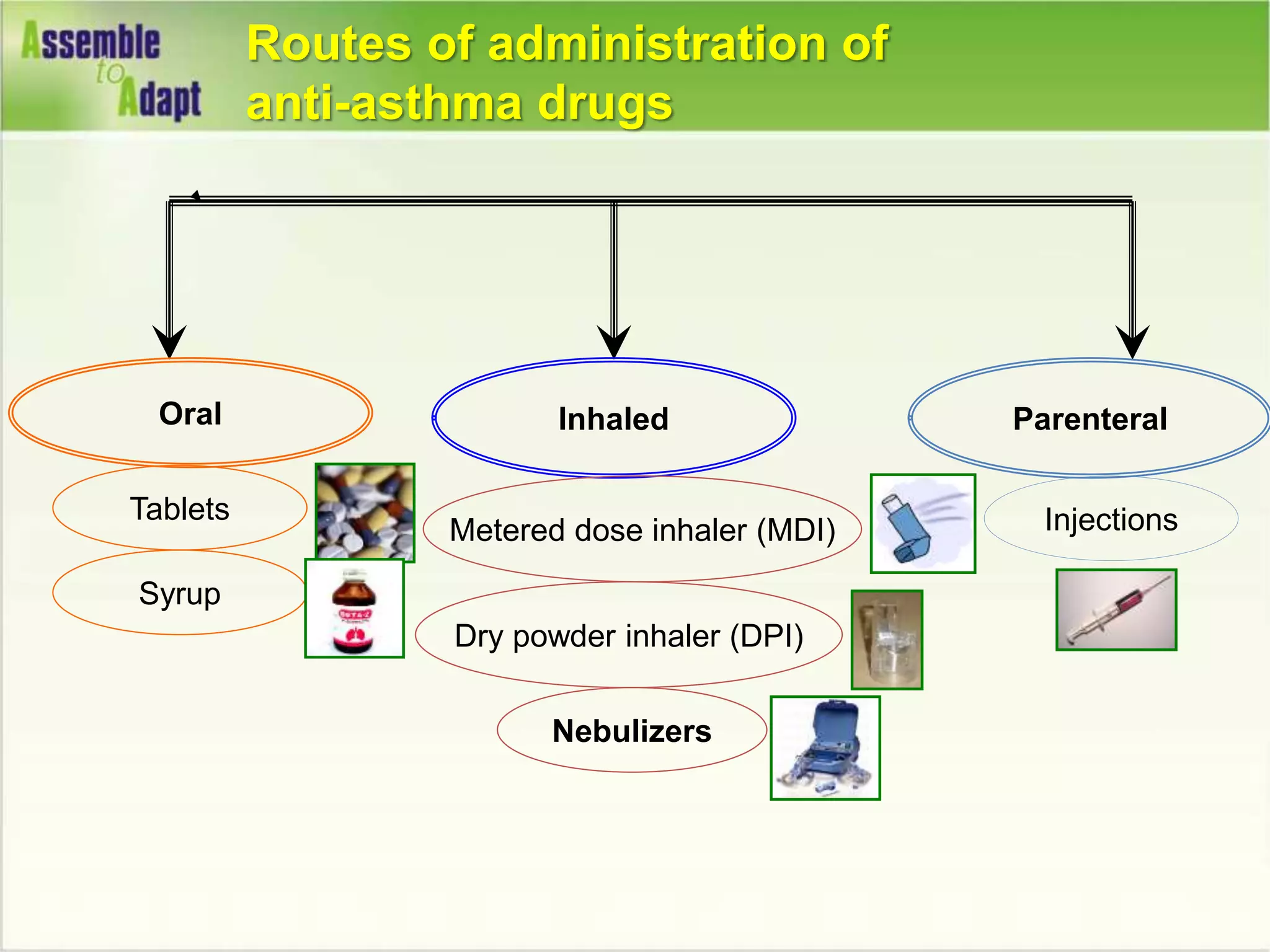
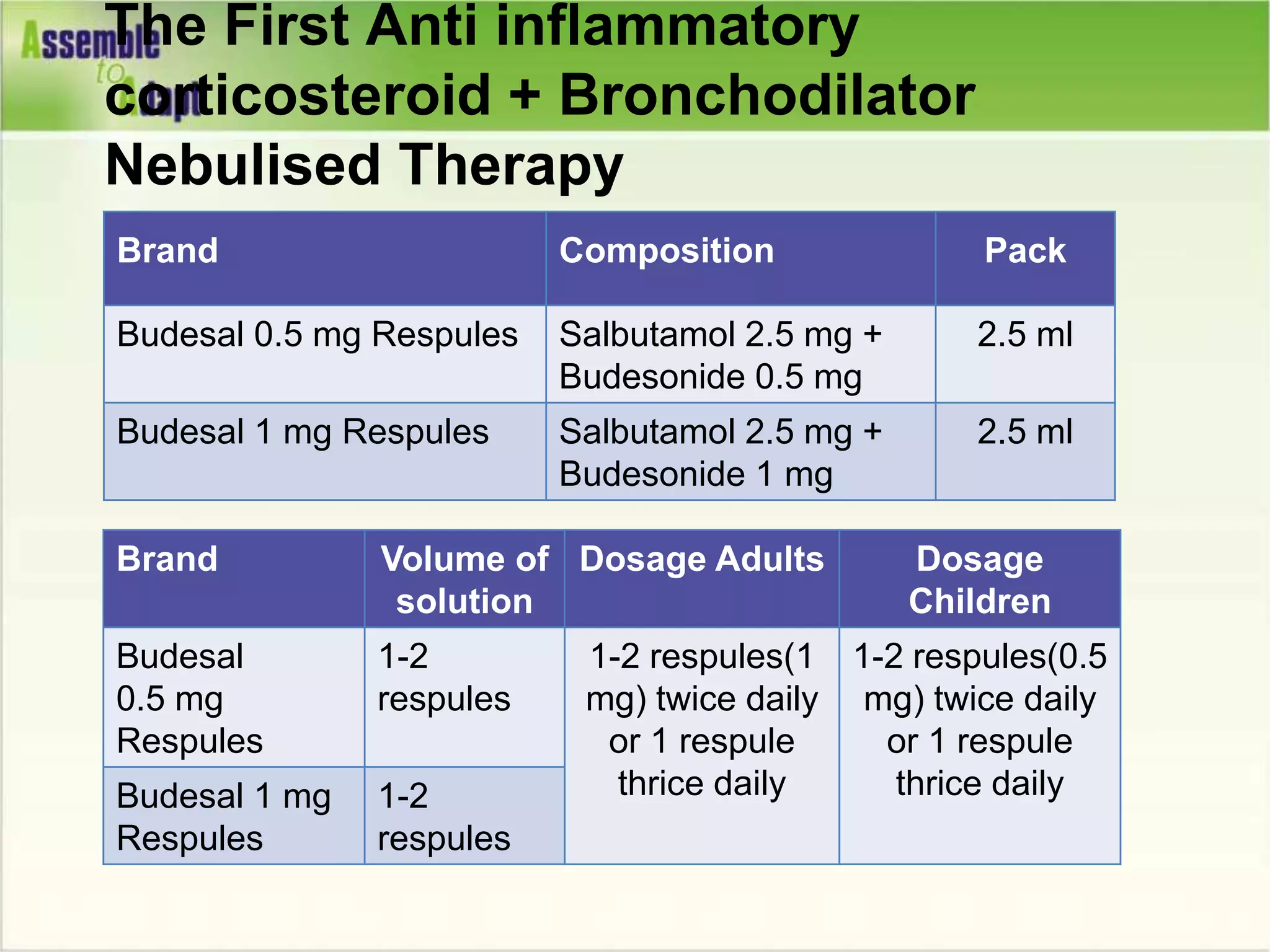
NEBULIZED [Respules/
Respirator solution]
MDI + SPACER
Salbutamol
[Asthalin]
Adult 2.5-5 mg Adult 8-12 puffs per hour
Child 1.25 -2.5 mg Child 4-6 puffs per hour
Levosalbutamol
[Levolin]
Adult 0.63-1.25 mg Adult 4-6 puffs per hour
Child 0.31-0.63 mg Child 2-3 puffs per hour](https://image.slidesharecdn.com/acuteasthmappt-230107072745-2fe21f3d/75/Acute-Asthma-PPT-ppt-25-2048.jpg)



![If patient has…
• Reduced distress
• Able to complete sentence
• Near normal Pulse rate/ respiratory rate
• No use of accessory muscles
• Improved Oxygen saturation
[>95%=Child / >90%=Adult]
Consider sending home](https://image.slidesharecdn.com/acuteasthmappt-230107072745-2fe21f3d/75/Acute-Asthma-PPT-ppt-29-2048.jpg)








![If patient has…
• No distress
• Able to complete sentence
• Near normal Pulse rate/ respiratory rate
• No use of accessory muscles
• Oxygen saturation [>95%=Child / >90%=Adult]
• Improved lung function [greater than 80% of predicted or
personal best]
Consider sending home](https://image.slidesharecdn.com/acuteasthmappt-230107072745-2fe21f3d/75/Acute-Asthma-PPT-ppt-39-2048.jpg)

![Other bronchodilators…
Theophylline
• Much less effective than Salbutamol + Ipratropium
• Injectible should be used in hospital settings only, with
monitoring serum levels.
• Mainly used as an add on therapy for prevention.
[long acting oral preparation]
Adrenaline
• Not routinely indicated for asthma attacks; mainly
indicated for anaphylaxis.](https://image.slidesharecdn.com/acuteasthmappt-230107072745-2fe21f3d/75/Acute-Asthma-PPT-ppt-41-2048.jpg)
![Do’s
• Never delay transfer to hospital/ICU if necessary
• Try to check pulse oximeter saturations at every step
• Ensure the patient who has been hospitalized is
discharged with regular ICS.
• Ensure patient has written asthma action plan.
• Prevent future acute asthma attacks by prescribing
regular treatment with inhaled corticosteroid
[MDI/ DPI].](https://image.slidesharecdn.com/acuteasthmappt-230107072745-2fe21f3d/75/Acute-Asthma-PPT-ppt-42-2048.jpg)